Nursing Exam Notes
MODULE 5 - MECHANISMS OF SELF-DEFENSE - CHAPTERS 7 – 10
Common the terms include:
- Self refers to particles, such as proteins and other molecules that are a part of, or made by your body. Something that is self should not be targeted and destroyed by the immune system. The non-reactivity of the immune system to self particles is called tolerance.
- Non-self refers to particles that are not made by your body, and are recognized as potentially harmful. These are sometimes called foreign bodies. Non-self particles or bodies can be bacteria, viruses, parasites, pollen, dust, and toxic chemicals.
- Antigens are anything that causes an immune response.
- Cytokines are molecules that are used for cell signaling, or cell-to-cell communication. Cytokines are similar to chemokines, wherein they can be used to communicate with neighboring or distant cells about initiating an immune response. Cytokines are also used to trigger cell trafficking, or movement, to a specific area of the body.
- Chemokines are a type of cytokines that are released by infected cells. Infected host cells release chemokines in order to initiate an immune response, and to warn neighboring cells of the threat.
Chapter 7: Innate Immunity
The innate immune system is the first line of defense. It is made of defenses against infection that can be activated immediately once a pathogen attacks. The innate immune system is essentially made up of barriers that aim to keep viruses, bacteria, parasites, and other foreign particles out of your body or limit their ability to spread and move throughout the body. The innate immune system is activated by the presence of antigens and their chemical properties.
The innate immune system includes:
- Physical Barriers- such as skin, the gastrointestinal tract, the respiratory tract, the nasopharynx, cilia, eyelashes and other body hair.
- Defense Mechanisms- such as secretions, mucous, bile, gastric acid, saliva, tears, and sweat.
- General Immune Responses- such as inflammation, complement, and non-specific cellular responses. The inflammatory response actively brings immune cells to the site of an infection by increasing blood flow to the area.
Cells of the Innate Immune System
There are many types of white blood cells or leukocytes that work to defend and protect the human body. In order to patrol the entire body, leukocytes travel by way of the circulatory system.
The following cells are leukocytes of the innate immune system:
- Phagocytes or Phagocytic cells: Phagocyte means “eating cell”, which describes what role phagocytes play in the immune response. Phagocytes circulate throughout the body, looking for potential threats, like bacteria and viruses, to engulf and destroy.
- Macrophages: Commonly abbreviated as “Mφ”, are efficient phagocytic cells that can leave the circulatory system by moving across the walls of capillary vessels. Macrophages can also release cytokines in order to signal and recruit other cells to an area with pathogens.
- Mast cells: Are found in mucous membranes and connective tissues, and are important for wound healing and defense against pathogens via the inflammatory response. When mast cells are activated, they release cytokines and granules that contain chemical molecules to create an inflammatory cascade. Mediators, such as histamine, cause blood vessels to dilate, increasing blood flow and cell trafficking to the area of infection. The mast cell is the most important activator of the inflammatory response.
- Neutrophils: Are phagocytic cells that are also classified as granulocytes because they contain granules in their cytoplasm. These granules are very toxic to bacteria and fungi, and cause them to stop proliferating or die on contact.
- Eosinophils: Are granulocytes targeting multicellular parasites. Eosinophils secrete a range of highly toxic proteins and free radicals that kill bacteria and parasites.
- Basophils: Are also granulocytes that attack multi-cellular parasites. Basophils release histamine, much like mast cells.
- Natural Killer cells: Natural Killer cells (NK cells), do not attack pathogens directly. Instead, natural killer cells destroy infected host cells in order to stop the spread of an infection.
- Dendritic cells: Antigen-presenting cells that are located in tissues, and can contact external environments through the skin, the inner mucosal lining of the nose, lungs, stomach, and intestines. Since dendritic cells are located in tissues that are common points for initial infection, they can identify threats and act as messengers for the rest of the immune system by antigen presentation. Dendritic cells also act as bridge between the innate immune system and the adaptive immune system.
Inflammation
Inflammatory Response (Second Line of Defense)
Inflammation is a biochemical and cellular process that occurs in vascularized tissues. Any break in the skin will allow bacteria to enter the body. These foreign microbes will cause swelling and reddening at the site of injury. This reaction by the body is called an inflammatory reaction or inflammatory response. It is caused by a variety of materials such as infection, mechanical damage, ischemia, nutrient deprivation, temperature extremes, radiation, etc.
Vascular response includes vasodilation (VD), blood vessels become leaky, and WBCs adhere to inner walls of vessels & migrate through the vessel
- Swelling, redness, heat, and pain: Inflammation is characterized by swelling, redness, heat, pain and dysfunction of the organs involved. When an injury occurs, a capillary and several tissue cells are apt to rupture, releasing histamine and kinins causing the capillaries to dilate, become more permeable, and leak fluid into these tissues. Dilation and fluid leaking into the tissues causes swelling, redness, and heat.
Phases of inflammation and Repair
- Cellular Injury
- Acute inflammation that involves healing
- Chronic Inflammation which also involves healing
- Granulation
- Healing
Unlike the immune system which is antigen-specific and has memory, the inflammatory response is non-specific because it takes place in about the same way no matter what the stimulus and occurs in the same manner even on second exposure to the same stimulus. Unlike chronic inflammation, the acute response is self-limiting; that is, it continues only until the threat to host is eliminated. This takes about 8 to 10 days, from the onset to healing. Inflammation is considered chronic if it is persists longer than 2 hours.
In the inflammatory process, cellular injury leads to acute inflammation, which may result in resolution and healing of the impaired site or progress into chronic inflammation. Chronic inflammation in turn results in either healing or progress into development of granuloma. The final step of the process is usually healing and reconstruction of the damaged tissue.
- Phagocytosis by neutrophils and macrophages: In the event of a break in the skin, neutrophils, monocytes (and macrophages) arrive and attempt to engulf and destroy the invaders. Phagocytosis is receptor-mediated event, which ensures that only unwanted particles are ingested.
- Stimulated macrophages can bring about an explosive increase in the number of leukocytes by producing Colony Stimulating Factors (CSFs). The CSFs pass by way of the blood to the bone marrow, where they stimulate the production and the release of white blood cells (WBCs), primarily neutrophils.
-Lymphocytes in nearby lymph nodes produce specific antibodies to attack the microbes. During the conflict, some neutrophils die and become mixed with dead tissue, bacteria, living white cells, etc. This thick yellow-white fluid is called pus.
The Complement System (Second line of Defense)
The complement system is a mechanism that complements other aspects of the immune response. Typically, the complement system acts as a part of the innate immune system, but it can work with the adaptive immune system if necessary.
The complement system is made of a variety of proteins that, when inactive, circulate in the blood. When activated, these proteins come together to initiate the complement cascade, which starts the following steps:
- Opsonization: Is a process in which foreign particles are marked for phagocytosis.
- Chemotaxis: Is the attraction and movement of macrophages to a chemical signal. Chemotaxis uses cytokines and chemokines to attract macrophages and neutrophils to the site of infection, ensuring that pathogens in the area will be destroyed.
- Cell Lysis: Lysis is the breaking down or destruction of the membrane of a cell. The proteins of the complement system puncture the membranes of foreign cells, destroying the integrity of the pathogen.
Agglutination: Uses antibodies to cluster and bind pathogens together, much like a cowboy rounds up his cattle. By bringing as many pathogens together in the same area, the cells of the immune system can mount an attack and weaken the infection.
8. Adaptive Immunity
The adaptive immune system, also called acquired immunity, is the third line of defense that uses specific antigens to strategically mount an immune response. Unlike the innate immune system, which attacks only based on the identification of general threats, the adaptive immunity is activated by exposure to pathogens, and uses an immunological memory to learn about the threat and enhance the immune response accordingly. The adaptive immune response is much slower to respond to threats and infections than the innate immune response, which is primed and ready to fight at all times.
Unlike the innate immune system, the adaptive immune system relies on fewer types of cells to carry out its tasks: B cells and T cells.
Both B cells and T cells are lymphocytes that are derived from specific types of stem cells, called multi-potent hematopoietic stem cells, in the bone marrow.
B cells
When a naive B cell encounters an antigen that fits or matches its membrane-bound antibody, it quickly divides in order to become either a memory B cell or an effector B cell, which is also called a plasma cell. Antibodies can bind to antigens directly.
The antigen must effectively bind with a naive B cell’s membrane-bound antibody in order to set off differentiation, or the process of becoming one of the new forms of a B cell.
B cells also express a specialized receptor, called the B cell receptor (BCR). B cell receptors assist with antigen binding, as well as internalization and processing of the antigen. B cell receptors also play an important role in signaling pathways.
T cells
All T cells express T cell receptors, and either CD4 or CD8, not both. So, some T cells will express CD4, and others will express CD8.
Unlike antibodies, which can bind to antigens directly, T cell receptors can only recognize antigens that are bound to certain receptor molecules, called Major Histocompatibility Complex class 1 (MHCI) and class 2 (MHCII). CD4 and CD8 play a role in T cell recognition and activation by binding to either MHCI or MHCII.
T cell receptors have to undergo a process called rearrangement, causing the nearly limitless recombination of a gene that expresses T cell receptors.
Mature T cells should recognize only foreign antigens combined with self-MHC molecules in order to mount an appropriate immune response.
T cells will undergo two selection processes:
- Positive selection ensures MHC restriction by testing the ability of MHCI and MHCII to distinguish between self and non-self proteins.
- Negative selection tests for self tolerance. Negative selection tests the binding capabilities of CD4 and CD8 specifically.
These two selection processes are put into place to protect your own cells and tissues against your own immune response. Without these selection processes, autoimmune diseases would be much more common.
After positive and negative selection, we are left with three types of mature T cells: Helper T cells, Cytotoxic T cells, and T regulatory cells.
- Helper T cells express CD4, and help with the activation of T cells, B cells, and other immune cells.
- Cytotoxic T cells express CD8, and are responsible for removing pathogens and infected host cells.
- T regulatory cells express CD4 and another receptor, called CD25. T regulatory cells help distinguish between self and non-self molecules, and by doing so, reduce the risk of autoimmune diseases.
|
Attribute |
Innate Immunity |
Adaptive Immunity |
|---|---|---|
|
Response Time |
Fast: minutes or hours |
Slow: days |
|
Specificity |
Only specific for molecules and molecular patterns associated with general pathogens or foreign particles |
Highly specific! Can discriminate between pathogen vs. non-pathogen structures, and miniscule differences in molecular structures |
|
Major Cell Types |
Macrophages, Neutrophils, Natural Killer Cells, Dendritic Cells, Basophils, Eosinophils |
T cells, B cells, and other antigen presenting cells |
|
Key Components |
Antimicrobial peptides and proteins, such as toxic granules |
Antibodies |
|
Self vs. Nonself Discrimination |
Innate immunity is based on self vs. nonself discrimination, so it has to be perfect |
Not as good as the innate immune system, but still pretty good at determining which is which. Problems in self vs. nonself discrimination result in autoimmune diseases |
|
Immunological Memory |
None |
Memory used can lead to faster response to recurrent or subsequent infections |
|
Diversity and Customization |
Limited: Receptors used are standard and only recognize antigen patterns. No new receptors are made to adapt the immune response |
Highly diverse: can be customized by genetic recombination to recognize epitopes and antigenic determinants. |
9. Alterations in Immunity and Inflammation
The immune system is a finely tuned network that protects the host against foreign antigens, particularly infectious agents. Sometimes this network breaks down, causing the immune system to react inappropriately.
Hypersensitivity: Allergy, Autoimmunity, and Alloimmunity
Hypersensitivity is an altered immunologic response to an antigen that results in disease or damage to the host.
Allergy is the deleterious effects of hypersensitivity to environmental antigens, and immunity means the protective responses to antigens expressed by disease-causing agents.
Autoimmunity is a disturbance in the immunologic tolerance of self-antigens.
Autoimmune diseases occur when the immune system reacts against self-antigens to such a degree that the person’s own tissues are damaged by autoantibodies or autoreactive T cells.
Alloimmunity occurs when the immune system of one individual produces an immunologic reaction against tissues of another individual.
Mechanisms of Hypersensitivity
Diseases caused by hypersensitivity reactions can be characterized also by the particular immune mechanism that results in the disease. These mechanisms are apparent in most hypersensitivity reactions and have been divided into four distinct types: type I (immunoglobulin E [IgE]–mediated) hypersensitivity reactions, type II (tissue-specific) hypersensitivity reactions, type III (immune complex–mediated) hypersensitivity reactions, and type IV (cell-mediated) hypersensitivity reactions.
The four mechanisms are interrelated, and in most hypersensitivity reactions, several mechanisms can be at work simultaneously or sequentially.
Immunologic Mechanisms of Tissue Destruction

Immune Complex Disease
Immune complex formation is dynamic as variations in the ratio of antigen to antibody, the class and subclass of antibody, and the quantity and quality of circulating antigen occur. At times the individual’s blood may become hypocomplementemic (i.e., contains below normal amounts of complement activity). During type I, II, or IV hypersensitivity reactions, complement levels are unaffected, or some components of the complement cascade, such as C3, may even be increased. Two prototypic models of type III hypersensitivity help explain the variety of diseases in this category.
Serum sickness- Is a model of systemic type III hypersensitivities. The systemic prototype of immune complex – mediated disease is called serum sickness because it was initially described as being caused by the therapeutic administration of foreign serum, such as horse serum that contained antibody against tetanus toxin. Serum sickness – type reactions are caused by the formation of immune complexes in the blood and their subsequent generalized deposition in target tissues.
Arthus Reaction- Is the prototypic example of a localized immune complex – mediated inflammatory response. It is caused by repeated local exposure to an antigen that reacts with preformed antibody and forms immune complexes in the walls of the local blood vessels. Symptoms of an Arthus reaction begin within 1 hour of exposure and peak 6 to 12 hours later. The lesions are characterized by a typical inflammatory reaction, with increased vascular permeability, an accumulation of neutrophils, edema, hemorrhage, clotting, and tissue damage.
Antigenic Targets of Hypersensitivity Reactions
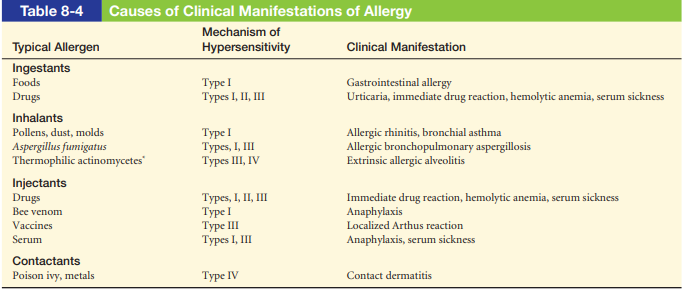
Allergy
Allergy is a hypersensitivity response against an environmental antigen (allergen). Although the most common allergies are type I hypersensitivities, any of the other three mechanisms may cause allergic responses. 19 Typical allergens that induce type I hypersensitivity include pollens (e.g., ragweed), molds and fungi (e.g., Penicillium notatum ), foods (e.g., milk, eggs, fi sh), animals (e.g., cat dander, dog dander), cigarette smoke, components of house dust (e.g., fecal pellets of house mites), and almost anything else we may encounter in our environment. Allergens that primarily elicit type IV allergic hypersensitivities include plant resins (e.g., poison ivy, poison oak), metals (e.g., nickel, chromium), acetylates and chemicals in rubber, cosmetics, detergents, and topical antibiotics (e.g., neomycin).
Urticaria, or hives, is a dermal (skin) manifestation of type I allergic reactions. The underlying mechanism is the localized release of histamine and increased vascular permeability, resulting in limited areas of edema.
Genetic Predisposition
Certain individuals are genetically predisposed to develop allergies, particularly type I allergies, and are called atopic. Atopic individuals tend to produce higher quantities of IgE and to have more Fc receptors for IgE on their mast cells.
Allergic Disease: Bee Sting Allergy
An example of a life-threatening allergy is an anaphylactic reaction to a bee sting. Bee venoms contain a mixture of enzymes and other proteins that may serve as allergens.
Autoimmunity is a breakdown of tolerance in which the body’s immune system begins to recognize self-antigens as foreign. It occurs when the immune system produces a response to tissues of another individual.
Sequestered Antigen- The induction of central tolerance requires that the self-antigen be present in the fetus and exposed to the developing fetal immune system.
Systemic lupus erythematosus (SLE)
Chronic multisystem inflammatory disease
Autoantibodies against: Nucleic acids, erythrocytes, coagulation proteins, phospholipids, lymphocytes, platelets, and many others
Deposition of circulating immune complexes containing antibody against the host’s Deoxyribonucleic acid (DNA)
More common in females
10. Infection
MODULE 6 - CELLULAR PROLIFERATION: CANCER - CHAPTERS 11-14
11. Stress and Disease
A person experiences stress when a demand exceeds a person’s coping abilities, resulting in reactions such as disturbances of cognition, emotion, and behavior that can adversely affect well-being.
I. Stressors: The Causes of Stress
A. Stress is defined as a complex set of reactions to real or perceived threats to one’s well being that motivates adaptation.
B. The sources or stimuli for stress are called stressors.
II. Frustration-Induced Stress
A. Frustration-induced stress results from the blocking or thwarting of goal-directed behavior.
- Environmental or social frustration refers to blocking of goal-directed behavior by something or somebody in the environment.
- Personal frustration results from internal or personal reasons.
B. Fault and blame are not relevant here.
III. Conflict-Induced Stress
A. A conflict is a stressor in which some goals can be satisfied only at the expense of others.
B. Four major types of motivational conflicts.
- Approach-approach conflicts result when a person is caught between two or more alternatives, each of which is positive or potentially reinforcing.
- With avoidance-avoidance conflicts, a person is faced with several alternatives, each of which is negative or punishing in some way.
- In approach-avoidance conflicts, there is only one goal a person would like to reach, but at the same time, would like to avoid.
- Multiple approach-avoidance conflicts result when a person is faced with a number of alternatives, each of which is in some way both positive and negative.
IV. Life-Induced Stress
A. In 1967, Holmes and Rahe published the first version of their Social Readjustment Rating Scale (SRRS).
- The scale provides a list of life events that might be potentially stressful.
- There is a positive correlation between scores on the SRRS and incidence of physical illness and disease.
B. While stress may predispose a person to physical illness, the scale does not demonstrate cause and effect outcomes.
V. Socioeconomic Status or SES
A. Socioeconomic status (SES) is a measure that reflects income, educational level, and occupation.
B. SES is related to stress in at least two ways.
- Persons of higher socioeconomic status are less likely than persons of low SES to encounter negative life events such as unemployment, poor housing, and less access to quality health care.
- Persons of low SES have fewer resources to deal with stressful life events when they do occur.
C. Richard Lazarus believes that stress is a result of life’s little hassles.
- Lazarus and his colleagues designed the Hassles Scale.
- This scale is a better predictor of symptoms such as anxiety and depression than the SRRS.
D. The Comprehensive Scale of Stress Assessment can be used with teens.
E. Stressors can be pleasant and desired, even though they may bring other hassles.
VI. Reacting to the Stressors in Our Lives
A. Stress is a reaction to stressors.
B. It motivates people to do something about the perceived threats to one’s well-being.
VII. Individual Differences in Responding to Stressors
- There are individual differences in how people respond to stressors.
- People who seem generally resistant to the negative aspects of stress have been labeled as having hardy personalities.
- Hardiness is related to the following three factors.
- Challenge
- Control
- Commitment
- Some researchers argue that there are sex differences in reacting to stress.
- Males are likely to show a “flight-or-flight” reaction.
- Females tend to exhibit “tend-and-befriend” reactions.
- Some responses to stress are more effective or adaptive than others.
VIII. Seyle’s General Adaptation Syndrome
A. The general adaptation syndrome or GAS refers to the physiological reactions one makes to stressors.
- The first response to the perception of a stressor is alarm, which activates the sympathetic division of the ANS.
- The second stage is resistance, where the drain on body resources continues.
- The third stage is exhaustion, when bodily resources become nearly depleted. B. Repeated exposure to stressors has cumulative effects.
IX. Effective Strategies for Coping with Stressors
A. There are several strategies to consider, including:
- Identify the stressor.
- Remove or negate the stressor.
- Reappraise the situation.
- Inoculate against future stressors.
- Take your time with important decisions.
- Learn techniques of relaxation.
- Engage in physical exercise.
- Seek social support.
B. Whereas the first five of the above may be thought of as problem-focused strategies, others deal more with the unpleasantness of experiencing stress, and are called emotion-focused strategies.
X. Ineffective Strategies for Coping with Stressors
A. Procrastination is a form of fixation—simply not doing something to remove the stressor.
B. Aggression is a maladaptive reaction to stressors.
- The frustration-aggression hypothesis claimed that aggression was always caused by frustration.
- It is now realized that there are other sources of aggression.
C. Anxiety is a general feeling of tension, apprehension, and dread that involves predictable physiological changes.
D. The anxiety that results from stress can become so discomforting and maladaptive to lead a psychologist to say that a person is suffering from a psychological disorder.
XI. Psychological Factors that Influence Physical Health
A. Health psychology is the field of applied psychology that studies psychological factors affecting physical health and illness.
- It may be that simply changing some “unhealthy behaviors” would be more effective and less expensive than treating illness or disease.
- Noting that biological factors (such as genetic predispositions) and psychological factors (such as a person’s reactivity to stressors) and social factors (such as the influence of family, social support, or one’s cultural expectations) all may interact to produce certain illnesses or diseases is called the biopsychosocial model.
B. There is a positive correlation between some personality variables and some aspects of physical health.
C. The Type A behavior pattern (TABP) originally was defined as describing a person who was competitive, achievement-oriented, impatient, easily aroused, often hostile and angry, who worked at many tasks at the same time.
- For nearly 20 years, many studies found a positive relationship between coronary heart disease (CHD) and behaviors typical of the Type A personality.
- Subsequent data failed to show a clear relationship between TABP and CHD.
- There may be a set of behaviors within the Type A behaviors that does predict CHD.
- It now seems that the active ingredients of TABP related to CHD are anger and hostility.
D. A person with a Type B behavior pattern is described as relaxed and easygoing.
E. More research is needed on adequately diagnosing TABP and its relationship to CHD.
XII. Why People Die: The Unhealthy Lifestyle
A. People die for an infinite number of reasons, but many deaths are premature and preventable.
- Nearly 2.5 million Americans die each year.
- Although death surely cannot be prevented, many deaths are premature and related to lifestyle choices.
B. Smoking, poor nutrition, obesity, and stress are behavioral risk factors that contribute to death.
C. Psychologists use behavioral techniques to promote healthy and safe behaviors.
XIII. SPOTLIGHT: Racial/Ethnic Disparities in Healthcare
- There are racial, ethnic, and gender disparities are three areas of healthcare:
- the incidence of disease and illness
- the quality of diagnostic and treatment services
- the availability and/or use of health insurance
- The incidence HIV/AIDS is higher among African Americans than any other ethnic group in the United States.
- African Americans are more likely to develop cancer than any other ethnic group.
- The rate of prostate cancer among African American males is 60 percent higher than the rate for Caucasian Americans.
- African American women have a significantly higher mortality for breast cancer than any other ethnic group.
- Asian Americans have a higher life expectancy than do members of any other ethnic group.
- Hispanic Americans are least likely than any other group to have health insurance benefits.
- Overwhelming evidence shows that racial and ethnic minorities are prone to poorer health care than white Americans, even when factors such as insurance status are controlled.
XIV. Helping People to Stop Smoking
- Cigarette smoking is responsible for over 440,000 deaths each year in the U.S and is associated with 5 million deaths a year worldwide.
- Most people who quit permanently do so without any special program of intervention.
- Using a nicotine patch in conjunction with therapy can be effective.
- Combining psychotherapeutic interventions with antidepressant medications seems promising.
- There has been some success with designing programs aimed at getting people to refrain from smoking in the first place.
- Increasing the taxes on cigarettes provides a negative incentive.
XV. Coping with HIV and AIDS
- Sexually transmitted diseases (STDs) are contagious diseases usually passed on through sexual contact.
- STDs affect millions of people each year, with 19,000,000 new cases reported each year in the United States.
- The human immunodeficiency virus, or HIV, causes acquired immune deficiency syndrome, or AIDS.
- The United Nations HIV/AIDS office estimates that 33.2 million people are living with HIV/AIDS worldwide.
- There currently is no vaccine to prevent AIDS.
- There is no cure, but some drug combinations can increase the life span and quality of life for those with the infection.
- The only reasonable way to avoid AIDS is through the careful monitoring of one’s behaviors.
- Successful interventions are multifaceted and involve:
- Education.
- Changing attitudes.
- Increasing motivation to engage in safer sexual practices.
- Providing people with negotiating skills.
- Targeting people most at risk.
- Marketing strategies.
- Knowledge of AIDS — in and of itself — is seldom useful in getting people to actually change their behaviors.
- Most teenagers simply do not believe that they will contract the HIV.
- As a result, most do not use condoms.
- A vaginal gel (Tenofir) has been shown to significantly reduce HIV transmission for the women who used it.
- A new and expensive medication (Truvada) has been shown to significantly reduce HIV infections among gay men who use it faithfully.
- AIDS has unprecedented psychological complications.
- Stress, depression, anger, anxiety, and denial are common.
- Males with AIDS are 7.5 times more likely to commit suicide than men in the general population.
- Others (even family members) often shun the AIDS patient.
12. Cancer Biology
What is Cancer?
Cancer can be defined as a disease in which a group of abnormal cells grow uncontrollably by disregarding the normal rules of cell division.
It is often presumed that all tumors are cancerous – but this is a misconception. A tumour becomes cancerous only when it spreads to other parts of the body
Types of Tumors
Benign Tumour
These tumors are localized at a particular location in the body. Moreover, it does not spread to the other parts of the body and is generally harmless. However, when a benign tumor occurs in areas such as the brain, they can turn fatal. Treatment often involves surgery and it does not grow back.
Malignant Tumor
These tumors are cancerous – meaning that it will grow quickly and spread to other normal tissues of the body. This ability to spread is called metastasis.
Premalignant Tumor
This type of tumor may be benign, but is observed to have the characteristics of a malignant tumor. It may not have metastasized yet, but it has the potential to turn cancerous. In other words, a premalignant tumor is a type of tumor that has an increased risk of becoming cancer. Benign tumors become premalignant and eventually, malignant.
Types of Cancer
Carcinoma
The most common form of cancer, it originates from the epithelial cells
Sarcoma
Originates from the connective tissues such as cartilage, fat and bone tissues
Melanoma
Originates from melanocytes, which are a type of cell that contains pigments
Lymphoma & Leukaemia
Originates from the cells that comprise blood (such as b lymphocytes or white blood cells)
Causes of Cancer
Many factors are attributed to causing cancer. The most probable factors include:
- Physical factors – Ionizing radiation, such as X-rays and gamma rays
- Chemical factors – Such as tobacco and smoke
- Biological factors – Viral oncogenes, proto-oncogenes and cellular oncogenes
The above factors are called carcinogens.
Diagnosis of Cancer
The detection and diagnosis of cancer are very important before it spreads to other parts of the body. Identification of cancer genes is pivotal to prevent cancer.
The following methods are used to detect cancer –
- Biopsy.
- Histopathological studies of tissue.
- Radiography technique.
- Computed tomography.
- Magnetic resonance imaging.
- Molecular biology techniques.
Treatment of Cancer
- Surgery – Surgically removing localized cancerous mass (Effective for benign tumours)
- Radiation therapy – In this therapy, radiation is used to kill the cancer cells.
- Chemotherapy – Chemotherapeutic drugs are used to kill cancer cells.
13. Cancer Epidemiology
Cancer epidemiology is the study of the pattern of cancer in populations. It’s essential aim is to identify causes of cancer, including preventable (avoidable) causes and inherited tumor susceptibility
Types of Epidemiologic Studies
- Descriptive Epidemiologic study: To describe the difference in occurrence of a particular cancer between different groups (age, gender, race, country, a period of time for time trend) and to generate the hypothesis for increased/decreased for the specific tumor type.
- Analytic Epidemiology: To study risk factors or potential causes of cancer by a particular study design, e.g., case-control study or cohorts study.
- Intervention studies: Applying the knowledge (risk/protective factors) obtained from analytic epidemiological studies to specific population in order to reduce the risk of cancer.
Risk factors for Cancer
- Tobacco Use: 30% (25%-40%)
- Infection: 10%? (1%-?)
- Reproductive & Sexual Behavior: 7% (1%-13%)
- Occupation: 4% (<2%-8%)
- Alcohol: 3% (2%-4%)
- Geophysical factors (natural radiation): 3% (2-4%)
- Pollution: 2% (<1% – 5%)
- Food additive: <1% (-5% – 2%)
- Medicines and Medical Procedures: 1% (0.5%-3%)
- Industrial consumer products <1% (<1%-2%)
- Diet in adult life, including obesity: 30%
- Sedentary lifestyle: 5%
- Defects in single genes that run in family: 5-10%
Chemical/environmental carcinogens
- Smoking and lung cancer
- Sun exposure and squamous cell carcinoma of skin
- Asbestos exposure and lung cancer
- Smoke food risk with nitrosamines and adenocarcinoma of the stomach
- Alcohol drinking and squamous cell carcinoma of esophagus
- Aflatoxin B1 and liver cancer
Radiation
- Exposure to ultraviolet radiation (in the form of sunlight) and squamous cell carcinoma of skin
- Ionizing radiation is related to skin cancer and leukemia in radiologist
Viral factors
- HPV (human papilloma virus) and Cervix cancer
- EBV(Epstein-Barr virus) and Nasopharyngeal cancer, Burkitt’s lymphoma
- HBV (hepatitis B virus) and hepatocellular carcinoma
- HIV (human immunodeficiency virus) and Kaposi’s sarcoma
Number of deaths for leading causes of death
Mortality by sex and cancer site, World
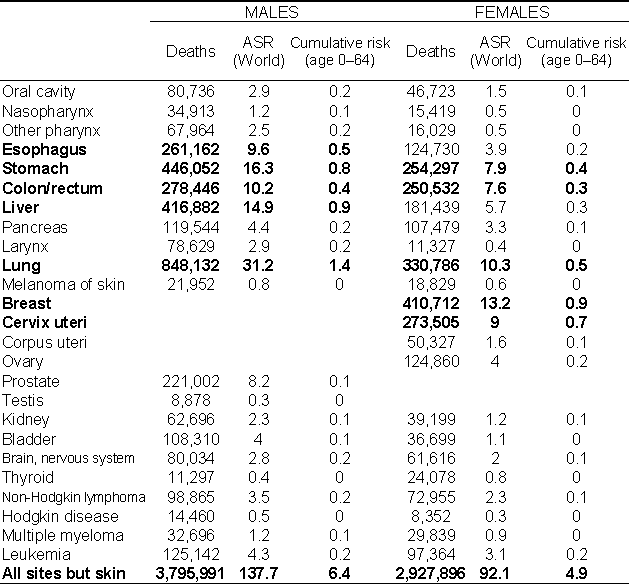
The Major Cancers
- Lung (ICD-10 C33 and C34)
- Breast (female, C50)
- Colon/rectum (C18-C20)
- Stomach (C16)
- Prostate (C61)
- Liver (C22)
- Cervix uteri (C53)
- Esophagus (C15)
14. Cancer in Children
Cancer is uncommon in children. Most cancers (99%) develop in adults, and it is most common in older adults. About 1 out of every 3 adults will develop cancer during his or her lifetime, while about 1 in 285 children will develop cancer before the age of 20.
What is childhood cancer?
Cancer in children can occur anywhere in the body, including the blood and lymph node systems, brain and spinal cord (central nervous system; CNS), kidneys, and other organs and tissues.
Cancer begins when healthy cells change and grow out of control. In most types of cancer, these cells form a mass called a tumor. A tumor can be cancerous or benign. A cancerous tumor is malignant, meaning it can grow and spread to other parts of the body. A benign tumor means the tumor can grow but will not spread to distant parts of the body.
In leukemia, a cancer of the blood that starts in the bone marrow, these abnormal cells very rarely form a solid tumor. Instead these cells crowd out other types of cells in the bone marrow. This prevents the production of:
- Normal red blood cells. Cells that carry oxygen to tissues.
- White blood cells. Cells that fight infection.
- Platelets. The part of the blood needed for clotting.
Most of the time, there is no known cause for childhood cancers. Childhood cancers may behave very differently from adult cancers, even when they start in the same part of the body.
Types of childhood cancer
Childhood cancer may also be called pediatric cancer.
Types of Cancer that Develop in Children
Leukemia
Leukemias, which are cancers of the bone marrow and blood, are the most common childhood cancers. The most common types in children are acute lymphocytic leukemia (ALL) and acute myeloid leukemia (AML). These leukemias can cause bone and joint pain, fatigue, weakness, pale skin, bleeding or bruising, fever, weight loss, and other symptoms. Acute leukemias can grow quickly, so they need to be treated (typically with chemotherapy) as soon as they are found.
Brain and spinal cord tumors
Brain and spinal cord tumors are the second most common cancers in children.
Most brain tumors in children start in the lower parts of the brain, such as the cerebellum or brain stem. They can cause headaches, nausea, vomiting, blurred or double vision, dizziness, seizures, trouble walking or handling objects, and other symptoms. Spinal cord tumors are less common than brain tumors in both children and adults.
Neuroblastoma
Neuroblastoma starts in early forms of nerve cells found in a developing embryo or fetus. This type of cancer develops in infants and young children. It is rare in children older than 10. The tumor can start anywhere, but it usually starts in the belly (abdomen) where it is noticed as swelling. It can also cause other symptoms, like bone pain and fever.
Wilms tumor
Wilms tumor (also called nephroblastoma) starts in one, or rarely, both kidneys. It is most often found in children about 3 to 4 years old, and is uncommon in older children and adults. It can show up as a swelling or lump in the belly (abdomen). Sometimes the child might have other symptoms, like fever, pain, nausea, or poor appetite.
Lymphomas
Lymphomas start in immune system cells called lymphocytes. These cancers most often start in lymph nodes or in other lymph tissues, like the tonsils or thymus. They can also affect the bone marrow and other organs. Symptoms depend on where the cancer starts and can include weight loss, fever, sweats, tiredness (fatigue), and lumps (swollen lymph nodes) under the skin in the neck, armpit, or groin.
The 2 main types of lymphoma are Hodgkin lymphoma (sometimes called Hodgkin disease) and non-Hodgkin lymphoma. Both types occur in children and adults.
Hodgkin lymphoma is more common, though, in early adulthood (usually in people in their 20s) and late adulthood (after age 55). Hodgkin lymphoma is rare in children younger than 5 years of age.
Non-Hodgkin lymphoma is more likely to occur in younger children than Hodgkin lymphoma, but it is still rare in children younger than 3. The most common types of non-Hodgkin lymphoma in children are different from those in adults. These cancers often grow quickly and require intense treatment, but they also tend to respond better to treatment than most non-Hodgkin lymphomas in adults.
Rhabdomyosarcoma
Rhabdomyosarcoma starts in cells that normally develop into skeletal muscles. This type of cancer can start nearly any place in the body, including the head and neck, groin, belly (abdomen), pelvis, or in an arm or leg. It may cause pain, swelling (a lump), or both. This is the most common type of soft tissue sarcoma in children.
Retinoblastoma
Retinoblastoma is a cancer of the eye that usually occurs in children around the age of 2, and is seldom found in children older than 6.
Normally when you shine a light in a child’s eye, the pupil looks red because of the blood in vessels in the back of the eye. In an eye with retinoblastoma, the pupil often looks white or pink.
Bone cancers
Cancers that start in the bones (primary bone cancers) occur most often in older children and teens, but they can develop at any age.
Two main types of primary bone cancers occur in children:
Osteosarcoma is most common in teens, and usually develops in areas where the bone is growing quickly, such as near the ends of the leg or arm bones. It often causes bone pain that gets worse at night or with activity. It can also cause swelling in the area around the bone.
Ewing sarcoma is a less common type of bone cancer. It is most often found in young teens. The most common places for it to start are the pelvic (hip) bones, the chest wall (such as the ribs or shoulder blades), or in the middle of the leg bones. Symptoms can include bone pain and swelling.
Risk Factors and Causes of Childhood Cancer
A risk factor is anything that increases the chances of getting a disease such as cancer. Different cancers have different risk factors.
Lifestyle and environmental risk factors
In adults, lifestyle-related risk factors, such as smoking, being overweight, not getting enough exercise, eating an unhealthy diet, and drinking alcohol play a major role in many types of cancer. But lifestyle factors usually take many years to influence cancer risk, and they are not thought to play much of a role in childhood cancers.
A few environmental factors, such as radiation exposure, have been linked with some types of childhood cancers.
Some studies have also suggested that some parental exposures (such as smoking) might increase a child’s risk of certain cancers, but more studies are needed to explore these possible links. So far, most childhood cancers have not been shown to have environmental causes.
Changes in genes
In recent years, scientists have begun to understand how certain changes in the DNA inside our cells can cause them to become cancer cells.
Cancers can be caused by DNA changes that keep oncogenes turned on, or that turn off tumor suppressor genes.
Inherited versus acquired gene mutations
Some children inherit DNA changes (mutations) from a parent that increase their risk of certain types of cancer. These changes are present in every cell of the child’s body, and they can often be tested for in the DNA of blood cells or other body cells. Some of these DNA changes are linked only with an increased risk of cancer, while others can cause syndromes that also include other health or developmental problems.
But most childhood cancers are not caused by inherited DNA changes. They are the result of DNA changes like acquired mutation that happen early in the child’s life, sometimes even before birth.
Acquired mutations are only in the person’s cancer cells and will not be passed on to his or her children.
Finding Cancer in Children
Screening for cancer in children
Screening is testing for a disease such as cancer in people who don’t have any symptoms. Childhood cancers are rare, and there are no widely recommended screening tests to look for cancer in children who are not at increased risk.
Possible signs and symptoms of cancer in children
- An unusual lump or swelling
- Unexplained paleness and loss of energy
- Easy bruising or bleeding
- An ongoing pain in one area of the body
- Limping
- Unexplained fever or illness that doesn’t go away
- Frequent headaches, often with vomiting
- Sudden eye or vision changes
- Sudden unexplained weight loss
Treating Children with Cancer
Treatment for childhood cancer is based mainly on the type and stage (extent) of the cancer. The main types of treatment used for childhood cancer are:
- Surgery
- Radiation therapy
- Chemotherapy (chemo)
The cancer treatment team
- Pediatric oncologists: doctors who specialize in using medicines to treat children with cancer
- Pediatric surgeons: doctors who specialize in performing surgery in children
- Radiation oncologists: doctors who specialize in using radiation to treat cancer
- Pediatric oncology nurses: nurses who specialize in caring for children with cancer
- Nurse practitioners (NPs) and physician assistants (PAs): nurses and other health professionals who are specially trained and licensed to practice medicine alongside doctors
Some of the possible late effects of cancer treatment include:
- Heart or lung problems (due to certain chemotherapy drugs or radiation therapy to the chest area)
- Slowed or delayed growth and development (in the bones or overall)
- Changes in sexual development and ability to have children
- Learning problems
- Increased risk of other cancers later in life
MODULE 7 - PULMONARY SYSTEM - CHAPTERS 35- 37
35. Structure and Function of the Pulmonary System
The pulmonary system is the network of organs and tissues that help one breathe. It includes the airways, lungs, and blood vessels. The muscles that power the lungs are also part of the pulmonary system. These parts work together to move oxygen throughout the body and clean out waste gases like carbon dioxide.
The act of breathing includes: inhaling and exhaling air in the body; the absorption of oxygen from the air in order to produce energy; the discharge of carbon dioxide, which is the byproduct of the process.
The parts of the respiratory system
Upper Respiratory Tract
Upper respiratory tract organs provide a route for air to move between the outside atmosphere and the lungs. They also clean, humidity, and warm the incoming air. However, no gas exchange occurs in these organs.
Nasal Cavity
The nasal cavity is a large, air-filled space in the skull above and behind the nose in the middle of the face. It is a continuation of the two nostrils. As inhaled air flows through the nasal cavity, it is warmed and humidified. Hairs in the nose help trap larger foreign particles in the air before they go deeper into the respiratory tract. In addition to its respiratory functions, the nasal cavity also contains chemoreceptors that are needed for the sense of smell and that contribute importantly to the sense of taste.
Pharynx
The pharynx is a tube-like structure that connects the nasal cavity and the back of the mouth to other structures lower in the throat including the larynx. The pharynx has dual functions: both air and food (or other swallowed substances) pass through it, so it is part of both the respiratory and the digestive systems. Air passes from the nasal cavity through the pharynx to the larynx (as well as in the opposite direction). Food passes from the mouth through the pharynx to the esophagus.
Larynx
The larynx connects the pharynx and trachea and helps to conduct air through the respiratory tract. The larynx is also called the voice box because it contains the vocal cords, which vibrate when air flows over them, thereby producing sound.
A very important function of the larynx is protecting the trachea from aspirated food. When swallowing occurs, the backward motion of the tongue forces a flap called the epiglottis to close over the entrance to the larynx. This prevents swallowed material from entering the larynx and moving deeper into the respiratory tract. If swallowed material does start to enter the larynx, it irritates the larynx and stimulates a strong cough reflex. This generally expels the material out of the larynx and into the throat.
Lower Respiratory Tract
The trachea and other passages of the lower respiratory tract conduct air between the upper respiratory tract and the lungs. These passages form an inverted tree-like shape, with repeated branching as they move deeper into the lungs. It is only in the lungs that gas exchange occurs between the air and the bloodstream.
Trachea
The trachea, or windpipe, is the widest passageway in the respiratory tract. It is about 2.5 cm wide and 10-15 cm long. It is formed by rings of cartilage, which make it relatively strong and resilient. The trachea connects the larynx to the lungs for the passage of air through the respiratory tract. The trachea branches at the bottom to form two bronchial tubes.
Bronchi and Bronchioles
There are two main bronchial tubes, or bronchi (singular, bronchus), called the right and left bronchi. The bronchi carry air between the trachea and lungs. Each bronchus branches into smaller, secondary bronchi; and secondary bronchi branch into still smaller tertiary bronchi. The smallest bronchi branch into very small tubules called bronchioles. The tiniest bronchioles end in alveolar ducts, which terminate in clusters of minuscule air sacs, called alveoli (singular, alveolus), in the lungs.
Lungs
The lungs are the largest organs of the respiratory tract. They are suspended within the pleural cavity of the thorax. The lungs are surrounded by two thin membranes called pleura, which secrete a fluid that allows the lungs to move freely within the pleural cavity. This is necessary so the lungs can expand and contract during breathing. Each of the two lungs is divided into sections called lobes, and they are separated from each other by connective tissues. The right lung is larger and contains three lobes. The left lung is smaller and contains only two lobes. The smaller left lung allows room for the heart, which is just left of the center of the chest.
Lung tissue consists mainly of alveoli. These tiny air sacs are the functional units of the lungs where gas exchange takes place. The two lungs may contain as many as 700 million alveoli, providing a huge total surface area for gas exchange to take place. Each time you breathe in, the alveoli fill with air, making the lungs expand. Oxygen in the air inside the alveoli is absorbed by the blood in the mesh-like network of tiny capillaries that surrounds each alveolus. The blood in these capillaries also releases carbon dioxide into the air inside the alveoli. Each time you breathe out, air leaves the alveoli and rushes into the outside atmosphere, carrying waste gases with it.
The lungs receive blood from two major sources. They receive deoxygenated blood from the heart. This blood absorbs oxygen in the lungs and carries it back to the heart to be pumped to cells throughout the body. The lungs also receive oxygenated blood from the heart that provides oxygen to the cells of the lungs for cellular respiration.
How the Respiratory System Works with Other Organ Systems
- The respiratory system works hand-in-hand with the nervous and cardiovascular systems to maintain homeostasis in blood gases and pH.
It is the level of carbon dioxide rather than the level of oxygen that is most closely monitored to maintain blood gas and pH homeostasis. The level of carbon dioxide in the blood is detected by cells in the brain, which speed up or slow down the rate of breathing through the autonomic nervous system as needed to bring the carbon dioxide level within the normal range. Faster breathing lowers the carbon dioxide level (and raises the oxygen level and pH); slower breathing has the opposite effects. In this way, the levels of carbon dioxide and oxygen, as well as pH, are maintained within normal limits.
- The pulmonary system also works closely with the cardiovascular system to maintain homeostasis.
The pulmonary system exchanges gases between the blood and the outside air, but it needs the cardiovascular system to carry them to and from body cells. Oxygen is absorbed by the blood in the lungs and then transported through a vast network of blood vessels to cells throughout the body where it is needed for aerobic cellular respiration. The same system absorbs carbon dioxide from cells and carries it to the respiratory system for removal from the body.
Function of the Pulmonary System
- Inhalation and Exhalation- Pulmonary Ventilation
The pulmonary system aids in breathing, also called pulmonary ventilation. In pulmonary ventilation, air is inhaled through the nasal and oral cavities (the nose and mouth). It moves through the pharynx, larynx, and trachea into the lungs. Then air is exhaled, flowing back through the same pathway. Changes to the volume and air pressure in the lungs trigger pulmonary ventilation. During normal inhalation, the diaphragm and external intercostal muscles contract and the ribcage elevates. As the volume of the lungs increases, air pressure drops and air rushes in. During normal exhalation, the muscles relax. The lungs become smaller, the air pressure rises, and air is expelled.
- External Respiration Exchanges Gases Between the Lungs and the Bloodstream
Inside the lungs, oxygen is exchanged for carbon dioxide waste through the process called external respiration. This respiratory process takes place through hundreds of millions of microscopic sacs called alveoli. Oxygen from inhaled air diffuses from the alveoli into pulmonary capillaries surrounding them. It binds to hemoglobin molecules in red blood cells, and is pumped through the bloodstream. Meanwhile, carbon dioxide from deoxygenated blood diffuses from the capillaries into the alveoli, and is expelled through exhalation.
- Internal Respiration Exchanges Gases Between the Bloodstream and Body Tissues
The bloodstream delivers oxygen to cells and removes waste carbon dioxide through internal respiration, another key function of the respiratory system. In this respiratory process, red blood cells carry oxygen absorbed from the lungs around the body, through the vasculature. When oxygenated blood reaches the narrow capillaries, the red blood cells release the oxygen. It diffuses through the capillary walls into body tissues. Meanwhile, carbon dioxide diffuses from the tissues into red blood cells and plasma. The deoxygenated blood carries the carbon dioxide back to the lungs for release.
Red blood cell
Red blood cells carry inhaled oxygen to the body's tissues and bring carbon dioxide back to the lungs to be exhaled.
- Air Vibrating the Vocal Cords Creates Sound
Phonation is the creation of sound by structures in the upper respiratory tract of the respiratory system. During exhalation, air passes from the lungs through the larynx, or “voice box.” When we speak, muscles in the larynx move the arytenoid cartilages. The arytenoid cartilages push the vocal cords, or vocal folds, together. When the cords are pushed together, air passing between them makes them vibrates, creating sound. Greater tension in the vocal cords creates more rapid vibrations and higher-pitched sounds. Lesser tension causes slower vibration and a lower pitch.
- Olfaction, or Smelling
The process of olfaction begins with olfactory fibers that line the nasal cavities inside the nose. As air enters the cavities, some chemicals in the air bind to and activate nervous system receptors on the cilia. This stimulus sends a signal to the brain: neurons take the signal from the nasal cavities through openings in the ethmoid bone, and then to the olfactory bulbs. The signal then travels from the olfactory bulbs, along cranial nerve 1, to the olfactory area of the cerebral cortex.
Protecting the Respiratory System
The respiratory system is well protected by the ribcage of the skeletal system. However, the extensive surface area of the respiratory system is directly exposed to the outside world and all its potential dangers in inhaled air.
The main way the respiratory system protects itself is called the mucociliary escalator. From the nose through the bronchi, the respiratory tract is covered in the epithelium that contains mucus-secreting goblet cells. The mucus traps particles and pathogens in the incoming air. The epithelium of the respiratory tract is also covered with tiny cell projections called cilia (singular, cilium), as shown in the figure below. The cilia constantly move in a sweeping motion upward toward the throat, moving the mucus and trapped particles and pathogens away from the lungs and toward the outside of the body.
The material that moves up the mucociliary escalator to the throat is generally removed from the respiratory tract by clearing the throat or coughing.
Coughing is a largely involuntary response of the respiratory system that occurs when nerves lining the airways are irritated. The response causes air to be expelled forcefully from the trachea, helping to remove mucus and any debris it contains (called phlegm) from the upper respiratory tract to the mouth. The phlegm may spit out (expectorated), or it may be swallowed and destroyed by stomach acids.
Sneezing is a similar involuntary response that occurs when nerves lining the nasal passage are irritated. It results in forceful expulsion of air from the mouth, which sprays millions of tiny droplets of mucus and other debris out of the mouth and into the air, as shown in the photo below. This explains why it is so important to sneeze into a sleeve rather than the air to help prevent the transmission of respiratory pathogens.
36. Alterations of Pulmonary Function
Normal breathing is called Eupnea - regular and rhythmic.
Common Signs and Symptoms of Respiratory Alteration
- Coughing - accumulation of secretions, irritating or destructive substances
- Dyspnea - lung/heart/neuromuscular causes (Subjective sensation of uncomfortable breathing. labored. Cough)
- Altered Breathing Patterns
- Apnea--- Bradypnea ---Tachypnea
- Hypoventilation --- Hyperventilation-- Kussmaul respirations (Increased rate and depth. Side effect of diabetic ketoacidosis.)
- Patterns - Cheyne-Stokes
Ventilation Determinants and Deterrents
NEED:
- patent airways with adequate diameter
- neuromuscular pump
- surfactant to reduce alveolar surface tension
REDUCED by:
- bronchospasm
- mucus plugs
- loss of elasticity
- thickening of airway
- trauma, anesthesia
- premature birth
- destruction of surfactant
PERFUSION OF LUNGS
NEED:
- Evenly distributed pulmonary blood flow
- Low pressure/low flow
- Match of V/Q
REDUCED by:
- Positional changes
- Obstruction - emboli
- Vasoconstriction
- Pulmonary hypertension
- Areas of poor ventilation
DIFFUSION
NEED:
- Partial pressure differences in gases
- Adequate surface area in alveoli
- Minimal distance for diffusion
REDUCED by:
- Low oxygen partial pressure
- Decreased area due to emphysema, lung cancer, deficient surfactant
- Pulmonary edema, exudate
GAS TRANSPORT
NEED:
- Partial pressure of oxygen above 80 mm in alveoli, arterial blood
- Hemoglobin and RBCs to transport gases
REDUCED by:
- Shifts in Hgb-O2 dissociation curve - Binding of Hgb-oxygen affected pH, pCO2, temp., 2,3DPG
- Hypoxemia
- Anemia
Common Questions
Cheyne stokes respirations?- Crescendo and decrescendo followed by apnea. Reduction of blood flow to the brainstem. Hypoxic component.
What is Paroxysmal nocturnal dyspnea?- Awakening at night and gasping for air; must sit up or stand up
What is Orthopnea?- Dyspnea when a person is lying down
What is Hemoptysis?- Coughing up blood or bloody secretions.
What is a protective reflex that clears airways by explosive expiration?- Cough.
What are the Signs & Symptoms of Pulmonary Disease?- Cough, Hemoptysis, Abnormal sputum.
What are Signs and Symptoms of Pulmonary Disease?- Hypoventilation and hyperventilation.
What occurs in Hypoventilation during pulmonary disease?- Alveolar ventilation is inadequate to the metabolic demands
-Leads to respiratory acidosis from hypercapnia
-Caused by airway obstruction, chest wall restriction
What occurs in Hyperventilation during pulmonary disease?- Alveolar ventilation exceeds the metabolic demands
-Leads to respiratory alkalosis from hypocapnia
-Caused by anxiety, head injury, severe hypoxemia
What is cyanosis?- Bluish discoloration of the skin and mucous membranes
When does cyanosis occur?- Develops when 5 g of hemoglobin is desaturated regardless of concentration
Sign of morphine is?- Respiratory depression.
What is Hypercapnia and why does it occur?- Increased CO2 in the arterial blood
Occurs from decreased drive to breathe or an inadequate ability to respond to ventilatory stimulation
What is the most common cause for perfusion abnormalities?- Shunting
Alveolar dead space: area where alveoli are ventilated but not perfused.
What occurs during Acute respiratory failure?- Gas exchange is inadequate (hypoxemia)
PaO2 ≤ 50 mm Hg
What occurs with a PACO2 greater than 50 and a Ph less than 7.25?- Hypercapnia
Low V/Q indicates?- Impaired ventilation followed by hypoxemia.
A shunt (very low) V/Q results in?- Blocked ventilation but continued perfusion. Collapsed alveolus and lung collapse. Hypoxemia occurs.
Impaired Perfusion causes?- Hypoxemia and High V/Q ratio. Pulmonary emobolis is a cause.
What is Flail chest?- When a portion of chest wall becomes unstable because of trauma to the ribcage or sternum.
What is Pneumothorax?- lung collapse due to air penetrating the pleural space.
What is pleural effusion?- Presence of fluid in pleural space
What is Empyema?- Infected pleural effusion
Pus in the pleural space.
complication in older adults or children due to surgery.
What is transudative effusion?- Watery and diffuses out of capillaries.
What is Exudative effusion?- Less watery and contains high concentrations of blood cells and plasma proteins
What is Hemothorax?- Blood exudate.
What are examples of Restrictive Lung Disorders?- Aspiration
-Atelectasis
-Bronchiectasis, bronchiolitis
-Pulmonary fibrosis
-Inhalation disorders
-Pneumoconiosis
-Allergic alveolitis
-Pulmonary edema
-Acute respiratory distress syndrome
What is aspiration?-Passage of fluid and solid particles into lungs
Right lower lobe most frequent site
What is Atelectasis?-Collapse of Lung tissue. can lead to shallow breathing.
What should nurses do for postoperative Atelectasis?-Prevention and treatment: Frequent turning, deep breathing, early ambulation, air humidification, and incentive spirometry
get patients up and moving. Use spirometer to promote good gas exchange.
What is Compression atelectasis?-external compression on the lung
Using a Spirometer can create enough pressure to open the?-Pore of Kohn.
What is Bronchiectasis?-Persistent abnormal dilation of the bronchi
Cylindrical, saccular, and varicose
Abnormal secretions in the alveoli creates an environment where?
Infection can spread.
What is Pulmonary fibrosis?-stiff lungs. Excessive amount of fibrous or connective tissue in the lung
-Idiopathic pulmonary fibrosis: no specific cause
-Exposure to toxic gases
What is oxygen toxicity?-Prolonged exposure to high concentrations of supplemental oxygen
Treatment for O2 toxicity?-reduce inspired oxygen to 60%
What happens with O2 toxicity?-Severe inflammatory response mediated primarily by oxygen radicals; damages alveolocapillary membranes, disrupts surfactant production, causes edema and decreased compliance
What can cause Inhalation disorders?-Exposure to toxic gases.
What is Pneumoconiosis?-Any change in lung caused by inhalation of organic dust particles, usually from workplace
Silica, asbestos, and coal: most common causes
What is Allergic Alveolitis?-Extrinsic allergic alveolitis (hypersensitivity pneumonitis)
Hypersensitivity to allergens; inhalation of organic dust particles or fumes. Causes lung inflammation.
When does pulmonary edema occur?-Changes in Capillary hydrostatic and capillary oncotic pressures
Fluid in the alveoli prevents?-gas exchange. and causes hypoxemia.
What king of heart failure can lead to PE?-Congestive heart failure.
Many ICU admissions are complicated by?-ARDS.
What are some Obstructive Pulmonary Disease?-Asthma
-Chronic bronchitis
-Emphysema
-Chronic bronchitis + emphysema = chronic obstructive pulmonary disease (COPD)
Main symptoms of OPD?-Dyspnea and wheezing
Asthma leads to?-Air trapping
Asthma is an?-Airway hyperresponsive problem. cascade because of allergen.
What is the 3rd leading cause of death in US?-COPD
What are risk factors for COPD?-tobacco smoke, occupational particulate exposure, pollution, and genetics.
What are the major events that lead to COPD?-Chronic bronchitis and Emphysema.
What is emphysema?-destruction o0f alveolar septs and loss of elastic recoil of bronchial walls.
What is chronic bronchitis?-bronchial edema, hypersecretion of mucus, bacterial colonization of airways.
What is difference between emphysema and chronic bronchitis?-loss of elastic recoil (emphysema) rather than mucus (Bronchitis).
What is the problem during emphysema?-exhalation.
What is 6th leading cause of death in US?-Pneumonia
What are adventitious sounds of Pneumonia?-signs of crackles, tactile fremitis
What are routes of infection for pneumonia?-Aspiration
-Inhalation
-Endotracheal tubes and suctioning
-Respiratory defenses cannot destroy microorganism
What is the leading cause of death from a curable infectious disease throughout the world?-Tuberculosis.
What is Tuberculosis?-Infection caused by Mycobacterium tuberculosis, an acid-fast bacillus
What are indicative of Respiratory tract infections?-Abscess
-Consolidation
-Cavitation
What is acute bronchitis and what are the symptoms?-Acute infection or inflammation of the airways or bronchi
-Commonly follows a viral illness
-Causes symptoms similar to pneumonia but does not demonstrate pulmonary consolidation and chest infiltrates
-Look at Virchows triad for the test.
What is Pulmonary Artery Hypertension?-Mean pulmonary artery pressure >25 mm Hg at rest
Idiopathic, familial, or associated
What causes Pulmonary Artery Hypertension?-Elevated left ventricular pressure
-Increased blood flow through the pulmonary circulation
-Obliteration or obstruction of the vascular bed
-Active constriction of the vascular bed produced by hypoxemia or acidosis
Pulmonary Artery Hypertension leads to?-vascular remodeling and Cor Pulmonale.
What is Cor Pulmonale?-Right ventricular enlargement
Cor Pulmonale causes?-Pulmonary hypertension, creating chronic pressure overload in the right ventricle
What is the manifestation of Cor Pulmonale?-Heart appears normal at rest but with exercise, decreased cardiac output, chest pain
Coughing is a protective reflex that expels secretions and irritants from the lower airway
Changes in the sputum volume, consistency, or color may indicate underlying pulmonary disease
Hemoptysis is expectoration of bloody mucus,
Abnormal breathing patterns are adjustments made by the body to minimize the work of respiratory muscles such as:
-Kussmaul, obstructed, restricted, gasping,
-Cheyne-Stokes respirations, and sighing.
Hypoventilation is decreased alveolar ventilation caused by airway obstruction, chest wall restriction, or altered neurologic control of breathing and causes increased partial pressure of carbon dioxide known as hypercapnia.
Hyperventilation is increased alveolar ventilation produced by anxiety, head injury, or severe hypoxemia and causes decreased partial pressure of carbon dioxide (known as hypocapnia)
Cyanosis is a bluish discoloration of the skin caused by desaturation of hemoglobin, polycythemia, or peripheral vasoconstriction.
Clubbing of the fingertips is associated with diseases that interfere with oxygenation of the tissues.
Chest pain can result from inflamed pleurae, tracheae, bronchi, or respiratory muscles.
Hypoxemia is a reduced partial pressure of blood oxygen caused by
a). decreased oxygen content of inspired gas,
b). hypoventilation,
c). diffusion abnormality,
d). ventilation-perfusion mismatch,
e). shunting.
Chest wall compliance is diminished by obesity and kyphoscoliosis, which compress the lungs, and by neuromuscular diseases that impair chest wall muscle function.
Flail chest results from rib or sternal fractures that disrupt the mechanics of breathing.
Pneumothorax is the accumulation of air in the pleural space. It can be caused by spontaneous rupture of weakened areas of the pleura or can be secondary to pleural damage caused by disease, trauma, or mechanical ventilation.
Tension pneumothorax is a life-threatening condition caused by trapping of air in the pleural space.
Pleural effusion is the accumulation of fluid in the pleural space resulting from disorders that promote transudation or exudation from capillaries underlying the pleura or from blockage or injury to lymphatic vessels that drain into the pleural space.
Atelectasis is the collapse of alveoli resulting from compression of lung tissue or absorption of gas from obstructed alveoli.
Bronchiectasis is abnormal dilation of the bronchi secondary to another pulmonary disorder, usually infection or inflammation.
Inhalation of noxious gases or prolonged exposure to high concentrations of oxygen can damage the bronchial mucosa or alveolo capillary membrane and cause inflammation or acute respiratory failure.
Pulmonary fibrosis is excessive connective tissue in the lung that diminishes lung compliance and may be idiopathic or caused by disease.
Bronchiolitis is the inflammatory obstruction of small airways. It is most common in children.
37. Alterations of Pulmonary Function in Children
Alterations of respiratory function in children are influenced by age, development, gender, race, genetic dominance, and environmental conditions. Newborns, premature newborns in particular, are especially vulnerable to a variety of upper and lower airway infections caused by immaturity of the airways, circulation, chest wall, and the immune system.
Structure and Function
A number of structural characteristics of the pulmonary system influence the way in which infants and children respond to respiratory disturbances.
Upper Airway
All conducting airways (the portions of airway that do not participate in gas exchange) are present at birth and change only in size throughout childhood. Branching of the bronchial tree is in fact complete by the sixteenth week of fetal life.
Because infants and children naturally have smaller-diameter airways than adults, they suffer more obstruction for a given degree of mucosal edema or secretion accumulation. The relative sizes of tonsils, adenoids, and epiglottis likewise are proportionately greater in the young child and with swelling can impose a significant site of obstruction. Infants up to 2 to 3 months of age are “obligatory nose breathers” and are unable to breathe in through their mouths. Nasal congestion is therefore a serious threat to a young infant.
Lower Airways and Lung Parenchyma
During fetal development the lung is transformed from a somewhat dense organ to one that is more delicately structured to facilitate air exchange. Beginning in the second trimester, there is loss of interstitial (mesenchymal) tissue with concomitant expansion of the future air spaces. Capillaries grow into the distal respiratory units that keep subdividing (alveolarization) to maximize surface area for gas exchange. The number of alveoli continues to increase during the first 5 to 8 years of life, after which the alveoli increase in size and complexity. In addition to the structural development of the lung in utero, there is accompanying functional maturation during which specialized cell types, such as type II cells, manifest.
Chest Wall Dynamics
Chest wall compliance is high in infants, particularly premature infants. The cartilaginous structures of the thoracic cage are not yet well ossified (ossification continues to occur throughout childhood), and the chest wall is easily collapsible. During inspiration in the young child, air is drawn in by the downward movement of the diaphragm, but the resulting negative pressure causes the “soft” chest wall to be drawn inward ; this produces so-called paradoxic breathing, or diaphragmatic breathing. Paradoxic breathing is especially seen during rapid eye movement (REM) sleep of premature infants. With pulmonary compromise the accessory muscles are drawn inward, creating retraction of the intercostal and supraclavicular spaces expand. In the face of an overly compliant chest wall, infants up to about 1 year of age are thought to maintain their FRC and avoid atelectasis by muscular “braking” of their expiration. This may occur either by active glottic narrowing or by increased activity of the inspiratory intercostal muscles.
Metabolic Characteristics
The basal metabolic rate of a child is greater than that of an adult, and thus oxygen consumption (VO2) is greater per unit of body weight. The VO2 of the child’s normal breathing accounts for up to 25% of the total VO2. The work of breathing increases VO2 exponentially with respiratory distress. Children have less muscle glycogen reserve, which limits the efficiency of accessory muscles, such that fatigue with lactic acidosis can occur quickly. Children also have a high proportion of extracellular fluid and therefore more quickly lose fluid and become dehydrated as a result of fever, from environmental heat, or in association with tachypnea (which causes evaporation from the respiratory tract).
Immunologic Incompetence
Passive immunity with immunoglobulin G (IgG) is normally conveyed transplacentally from the mother to the fetus beginning at 20 weeks of gestation; thus IgG levels are lower in preterm than term infants. Breast-feeding allows transfer of secretory IgA, IgG, and IgM after birth. Because IgG has a half-life of approximately 21 days, the placentally transferred antibodies are depleted after just a few months. Infants are able to synthesize IgG, IgM, and IgA, and the levels of these immunoglobulins increase slowly with age. Cell-mediated immunity is also not fully developed in the neonate, which creates a situation of enhanced susceptibility to viral and fungal infections.
Physiologic Control of Respiration
For up to 3 weeks of age, the newborn has a blunted ventilatory response to hypoxia compared with older children and adults. The mechanisms for this are not well understood but may reflect reduced activity of the peripheral chemoreceptors (in the carotid body) and nonadaptive responses in the respiratory center (in the brainstem). Ventilatory response to hypercarbia is normal in term infants but may be reduced in premature infants. Congenital or acquired lesions of the central nervous system may cause hypoventilation or apnea. Exposure to maternal smoking both during and after fetal development can have significant deleterious effects on lung development and subsequent susceptibility to pulmonary disorders.
Disorders of the Upper Airways
Pulmonary dysfunction can be categorized into disorders of either the upper airway or the lower airway. Signs of acute respiratory failure are the same regardless of etiology. These include the following:
- Increased respiratory effort with retractions or gasping (apnea in some conditions)
- Cyanosis or pallor
- Agitation
- Decreased level of consciousness
- Cardiovascular signs: tachycardia, mottled color, or bradycardia
- Physiologic compromise reflected by hemoglobin desaturation, hypoxemia, hypercarbia, and acidosis
Upper Airway Obstruction
The crucial issue in the upper airways is patency. The most common causes of acute-onset upper airway obstruction (UAO) in children are infections, foreign body aspiration, angioedema, obstructive sleep apnea, and trauma. Chronic UAO has many etiologies, including congenital malformations affecting the airway, cartilaginous weakness, vocal cord paralysis, and subglottic stenosis.
Causes of Upper Airway Obstruction In Children According To Site Of Obstruction
Nose and Pharynx
-Choanal atresia
-Lingual thyroid or thyroglossal cyst
-Macroglossia
-Micrognathia
-Hypertrophic tonsils/adenoids
-Retropharyngeal or peritonsillar abscess
Larynx
-Laryngomalacia
-Laryngeal web, cyst, or laryngocele
-Laryngotracheobronchitis (viral croup)
-Acute spasmodic laryngitis (spasmodic croup)
-Epiglottitis
-Vocal cord paralysis
-Laryngotracheal stenosis
-Intubation
-Foreign body
-Cystic hygroma
-Subglottic hemangioma
-Laryngeal papilloma
-Angioneurotic edema
-Laryngospasm (hypocalcemic tetany)
-Psychogenic stridor
Trachea
-Tracheal stenosis
-Tracheomalacia
-Bacterial tracheitis
-External compression
The site and nature of the obstruction are often discernible by assessing the noise associated with breathing, the quality of the voice or cry, and the presence of feeding difficulties.
Likewise, the severity of the problem often can be judged by visual observation of signs, including retractions, nasal flaring, gasping or obstructed breaths, anxiety, restlessness, or need to maintain a specific head or body position. Agitation should be regarded as a likely sign of hypoxemia or obstruction.
In acute UAO, increasing the child’s anxiety by excessive physical examination can worsen the condition. The child should be kept as calm as possible. The clinician should never attempt a pharyngeal examination if there is any suspicion of epiglottitis or retropharyngeal abscess because this maneuver may precipitate acute obstruction of the airway.
The sounds of the child’s breathing can provide key clues. A sonorous, snoring noise is typical for nasopharyngeal obstruction, such as adenotonsillar hypertrophy. A common sign of pediatric UAO is stridor, a harsh, vibratory sound of variable pitch caused by turbulent flow through the partially obstructed airway. Biphasic noise may sometimes mean abnormalities of both the extrathoracic and intrathoracic trachea (long-segment stenosis or malacia).
Abnormalities of voice or cry (weak or hoarse) suggest problems at the larynx, such as vocal cord paralysis.
Muffling of the voice, especially in an acute condition, suggests supralaryngeal obstruction, such as epiglottitis or retropharyngeal abscess. Pronounced cough may be an irritative symptom, such as that produced by an aspirated foreign body, or may be a sign of tracheal obstruction. The cough associated with croup or tracheal foreign body is usually harsh and barking.
Airway obstruction occurs sooner in infants than in older children. Obviously, airway luminal size is smaller in accordance with smaller body size, but any decrease in luminal diameter will be much more significant.
Infections
Infections of the upper airway are common in children; some have the potential to cause life-threatening emergencies. Recognition and rapid evaluation of these problems are crucial pediatric care skills.
Croup
Croup illnesses can be divided into two categories: (1) acute laryngotracheobronchitis (croup) and (2) spasmodic croup. Diphtheria can be considered a croup illness but is now rare because of vaccinations. Croup illnesses are all characterized by infection and obstruction of the upper airways.1
Croup is an acute laryngotracheobronchitis and most commonly occurs in children from 6 months to 3 years of age, with peak incidence at 2 years of age. In 85% of cases, croup is caused by a virus, most commonly parainfluenza; however, other viruses such as influenza A virus, respiratory syncytial virus (RSV), rhinovirus, adenovirus, and rubella virus (measles) as well as the atypical bacterium Mycoplasma pneumoniae has been associated with causation.
Croup is more common in boys than girls. In a significant portion of affected children, croup is a recurrent problem during childhood, and there is a family history of croup in about 15% of cases.
Spasmodic croup is characterized by similar hoarseness, barking cough, and stridor, but is of sudden onset, usually at night and without viral prodrome. It often resolves as quickly as it develops and usually occurs in older children. The etiology is unknown although association with viruses, allergies, asthma, and gastroesophageal reflux disease (GERD) is being investigated.3
Maternal Smoking: Fetal Lung Development and Lung Disease
Maternal smoking during pregnancy is a risk factor for several adverse developmental outcomes, including abnormal fetal lung development.
Respiratory failure is the same regardless of etiology. These include the following:
- Increased respiratory effort with retractions or gasping (apnea in some conditions)
- Cyanosis or pallor
- Agitation
- Decreased level of consciousness
- Cardiovascular signs: tachycardia, mottled color, or bradycardia
- Physiologic compromise reflected by hemoglobin desaturation, hypoxemia, hypercarbia, and acidosis
Upper Airway Obstruction
The crucial issue in the upper airways is patency. The most common causes of acute-onset upper airway obstruction (UAO) in children are infections, foreign body aspiration, angioedema, obstructive sleep apnea, and trauma.
Acute Epiglottitis
Acute epiglottitis is caused by Haemophilus influenzae type B (Hib). Since the advent of Hib immunization, the overall incidence of acute epiglottitis in children has decreased significantly, although Hib still accounts for approximately 25% of the cases seen in children. Infants less than 1 year of age are at greater risk.
Tonsillar Infections
Tonsillar infections (tonsillitis) are occasionally severe enough to cause UAO. As with other infections of the upper airway, the incidence of tonsillitis secondary to group A beta-hemolytic Streptococci (GABHS) and methicillin-resistant S. aureus (MRSA) has risen notably in the past 15 years. Significant swelling of the tonsils and pharynx occurs, and a tenacious membrane may cover the mucosa.
Peritonsillar abscess is usually unilateral and is most often a complication of acute tonsillitis.
Bacterial Tracheitis
Bacterial tracheitis is the most common potentially life-threatening upper airway infection in children. It is most often caused by Staphylococcus aureus (S. aureus) (including methicillin-resistant [MRSA] strains), H. influenzae, group A beta-hemolytic Streptococcus (GABHS [Streptococcus pyogenes]), or Moraxella catarrhalis.
Retropharyngeal Abscess
Retropharyngeal abscess can be caused by aerobic, anaerobic, or polymicrobial infection. A decrease in retropharyngeal abscess has been noted in the past several years that is likely related to the use of corticosteroids in the treatment of influenza and croup.
Retropharyngeal abscess usually occurs more commonly in male children about 4 years of age and as a consequence of either nasopharyngeal infection or penetrating local injury. Clinical signs include fever, dysphagia, drooling, stridor, respiratory distress, and stiff neck. This condition requires intravenous antibiotics targeted at the suspected microorganism, and sometimes incision and drainage.
Angioedema
Angioedema is a localized edema involving the deep, subcutaneous layers of skin or mucous membranes. Generally, angioedema causes facial swelling first, particularly around the eyes and lips, and may progress to airway swelling. Angioedema is usually secondary to allergic phenomena (e.g., allergy to peanuts, cow’s milk, chicken eggs).
Laryngomalacia and Tracheomalacia
Laryngomalacia results from abnormally soft laryngeal cartilages and is the most common cause of chronic stridor in infants. Boys are twice as likely as girls to present with symptoms.
Typical signs of laryngomalacia include inspiratory stridor beginning in the first days or weeks of life, accentuated with activity, and sometimes with positional changes (worse in supine or head-flexed positions). Feeding difficulties may be noted, but they are usually mild. Cry is normal.
Vocal Cord Paralysis
Vocal cord paralysis is second to laryngomalacias as a cause of stridor and is a relatively uncommon congenital disorder. The vocal cords should move apart to facilitate inspiration and move together to facilitate vocalization.
Subglottic Stenosis
Congenital subglottic stenosis is the third most common laryngeal anomaly and is defined as a subglottic airway diameter of less than 4 mm at the cricoid region in a full-term infant, and less than 3 mm in a premature infant. Incomplete recanalization of the laryngotracheal tube during the third month of gestation results in this defect. Subglottic stenosis also is associated with eosinophilic esophagitis, Wegener granulomatosis, and neurofibromatosis.
Obstructive Sleep Apnea Syndrome
Obstructive sleep apnea syndrome (OSAS) is a breathing disorder defined by prolonged partial and/or intermittent complete UAO during sleep with disruption of normal ventilation and normal sleep patterns. Childhood OSAS is common with an estimated prevalence of 2% to 3% among middle-school children and as many as 13% of children ages 3 to 6 years.
Respiratory Distress Syndrome of the Newborn
Respiratory distress syndrome (RDS) of the newborn (previously known as hyaline membrane disease [HMD]) is a major cause of neonatal morbidity and mortality. It occurs almost exclusively in premature infants and the incidence has increased in the United States over the past two decades. Preterm births account for about 12% of all births. Black mothers have 1.5 times the risk of preterm birth and 3.4 times the risk of preterm-related mortality. RDS occurs in 50% to 60% of infants born at 29 weeks of gestation and decreases significantly by 36 weeks. Infants of diabetic mothers and those with cesarean delivery (especially elective C-section) are more likely to develop RDS because the labor-associated catecholamine and steroid surge do not occur, causing decreased pulmonary surfactant release.78 It is more common in boys than girls. The major predisposing factor is prematurity because the immature lung is not well structured for gas exchange and has not yet developed adequate surfactant production and secretion.
