The linkage between growing older, increased exercise and the management of blood pressure
Type: Dissertation Literature Review
Subject: Healthy Ageing
Subject area: Nursing
Education Level: Masters Program
Length: 9 pages
Referencing style: Harvard - standard
Preferred English: UK English
Spacing Option: Double
School: Chamberlain University
Title: The linkage between growing older, increased exercise, and the Management of blood pressure
Chapter One: Background
Chapter One: introduction
This chapter provide an overview of cardiovascular disease, hypertension, exercise, and background to hypertension.
1.1 Background to cardiovascular disease
The prevalence of chronic health conditions is significantly increasing globally (Hajat and Stein, 2018). These can be attributed to various factors which increase an individual's risk of developing the disease. Some of these conditions require lifetime follow-up, with some resulting in potentially life-threatening complications. The regular follow-ups and medications required in managing these conditions are also resource-intensive, resulting in a financial burden to the affected patients as well as their families and friends (Hajat and Stein, 2018). Besides, the various chronic conditions affect the physical and mental health of affected patients, thereby resulting in poor quality of life (Hajat and Stein, 2018).
This paper focuses on cardiovascular diseases, one of the chronic health conditions and among the leading cause of death globally (Timmis et al., 2020). They include a wide range of conditions, such as coronary heart disease, cerebrovascular diseases, rheumatic heart diseases, congenital heart diseases, peripheral artery diseases, and deep venous thrombosis, which can complicate pulmonary embolism (Timmis et al., 2020). Stroke and heart attacks are often acute life-threatening events due to inadequate or blockage of blood supply to the brain and heart, respectively, although stroke can also occur due to bleeding of brain vessels (Battaglini et al., 2020). Like any other conditions, patients with cardiovascular diseases present with certain symptoms, including chest pain, dizziness, difficulty breathing, and syncopal attacks. Besides, certain risks expose an individual to a danger of developing these conditions, for instance, unhealthy diet, lack of physical activity, and harmful use of alcohol and tobacco smoking (Virani et al., 2021).
1.2 Global Statistics of Cardiovascular Diseases
Cardiovascular diseases are a global health concern, affecting millions of people regardless of their racial or ethnic backgrounds. According to the WHO (2021) report on non-communicable diseases of 11th June 2021, cardiovascular diseases were identified as the leading cause of death worldwide. Besides, in 2019, approximately 17.9 million were reported to have died from cardiovascular diseases, which corresponded to approximately 32% of total global deaths the same year (Timmis et al., 2020). 85% of all cardiovascular deaths were also due to heart attack and stroke (WHO, 2021). Additionally, more than 75% of the deaths were reported in low and middle-income countries (WHO, 2021). Of the 17 million premature deaths recorded in the same year, which implied death for those below 70 years due to non-communicable diseases, cardiovascular diseases were the leading contributor, with an estimated 38% of all deaths (Timmis et al., 2020).
According to the European Heart Journal, cardiovascular diseases contribute to approximately 34% of deaths in the Middle East, which is slightly above the global estimate of 32%. The journal also identifies dyslipidemia as a significant independent risk factor for developing cardiovascular disease in the Middle East (Sardarinia et al., 2016). Cardiovascular diseases were also responsible for almost half of deaths in Kuwait and Oman, with an estimated 46% and 49%, respectively. Other regions within the Middle East, such as Qatar, Bahrain, UAE, and Saudi Arabia, also recorded significant deaths due to cardiovascular diseases, with an estimate of 23%, 32%, 38%, and 42% of total deaths, respectively (Sardarinia et al., 2016). The high prevalence of cardiovascular diseases within the Middle East countries has been attributed to the rapid socioeconomic growth, which has resulted in a change in people's lifestyles.
Hypertension is also common in the Middle East, contributing to approximately 39% of all cardiovascular-related deaths in Lebanon and 28% in the UAE (Sardarinia et al., 2016). Other risk factors implicated in the high prevalence of cardiovascular diseases in the Middle East include diabetes, with 6 of the world’s top 10 nations with diabetes coming from the Middle East (Sardarinia et al., 2016). There is also a high prevalence of obesity, especially among the Middle East female population, and a high smoking prevalence among Jordanian males at 61%, ranked 8th globally. Research such as the INTERHEART and Gulf-RACE found that the prevalence of heart attack is higher and at a younger age, ranging from 45 to 50 among patients in the Middle East, which is 10 to 12 years earlier compared to their counterparts in the West (Sardarinia et al., 2016). Such statistics show why this issue is a major concern for the Middle East population, given that it is expected to rise if no measures are put to address the risk factors.
1.3 Cardiovascular Disease's Effect on the Body and the Mortality Rate
As aforementioned, cardiovascular diseases are the leading cause of death globally. The British Heart Association explains how cardiovascular disease impact body functions and leads to death if not adequately addressed. A good function circulatory system is essential for survival. When one develops diseases affecting the circulatory system, they have cardiovascular diseases (Timmis et al., 2020). This, therefore, limits tissue perfusion and waste removal from the body, hence affecting normal functioning. When blood vessels supplying vital organs such as the heart or brain are affected, the patient is at risk of developing a heart attack or stroke, which are life-threatening and form the commonest cause of death in patients with cardiovascular conditions (Timmis et al., 2020). Other organs, such as the kidneys, may also be affected in the long run, hence death due to renal failure.
1.4 Bloop pressure and hypertension management
The American Society of Hypertension considers individuals with optimal blood pressure and no early signs of cardiovascular disease to be normal (Pickering et al., 2008). On the other hand, the European Society of Cardiology (2018) suggest that there is a strong continuous correlation between blood pressure (BP) and cardiovascular, so the distinction between normotension and hypertension based upon cut-off BP values seems somewhat arbitrary(Modesti et al.). It has been proven that BP and CV risk are epidemiologically associated even at very low levels of blood pressure like for systolic blood pressure (SBP) >115 mmHg (Williams et al., 2018). The term hypertension, however, refers to the level of BP at which lifestyle interventions or drugs are found to have more significant benefits than risks, as documented in clinical trials (Williams et al., 2018). Accordingly, there are now three types of blood pressure: normal, elevated, and stage 1 or 2 hypertension. Elevated blood pressure is defined as 120-129/80 mmHg, while normal blood pressure is 120/80 mmHg. In stage one, the systolic blood pressure (SBP) is 130-139 mmHg, and the diastolic blood pressure (DBP) is 80-89 mmHg. In stage 2 hypertension, blood pressure is at or above 140 mmHg and/or diastolic blood pressure is at or above 90 mmHg. According to the Systolic Blood Pressure Intervention Trial (SPRINT), a target of 130 mmHg for most adults aged 65 and over is recommended (National Heart Lung Blood Institute, 2011).
Relating to the leading factors that may cause hypertension, it can be classified into two types primary or essential hypertension and secondary HTN accounting for ninety-five percent and five percent of hypertensive individuals, respectively (Weber et al., 2014). In addition, it is vital to note that each type has its cause. Despite the lack of knowledge about the aetiology of essential hypertension, it typically develops in the fifth or sixth decade of life(Weber et al., 2014). It is associated with increased salt intake and obesity and is strongly associated with family history, suggesting a genetic predisposition to developing the disease (Saxena et al., 2018). In contrast, secondary HTN may also be accompanied by secondary causes such as renal artery stenosis, chronic kidney disease, sleep apnea, and adrenal disease (Weber et al., 2014).
Also Read:Nursing Dissertation Writing Service
The body tightly regulates the blood pressure for normal functioning. Other factors, however, contribute to hypertension, which is also a leading risk factor for the development of cardiovascular diseases (Fuchs and Whelton, 2020). Age is one of the non-modifiable risk factors for the development of hypertension (Fuchs and Whelton, 2020). One of the modifiable factors is an individual’s weight, which can significantly help prevent hypertension or even aid in its management. Exercise helps in ensuring a healthy body weight, and in improving the health of the blood vessels and the heart, thus enabling them to function efficiently. With time, exercise helps lower the resting heart rate and blood pressure, which is healthy.
Through weight control, exercise can therefore help in blood pressure control (Fuchs and Whelton, 2020). Regular exercise can be as effective as antihypertensive in lowering blood pressure, with more advantages such as being affordable, accessible, and improving overall cardiovascular (Fuchs and Whelton, 2020). A recent study recorded in the journal of the American Heart Association (JAHA) on exercise training for blood pressure endurance and both isometric and dynamic resistance were helpful in a marked reduction in systolic blood pressure (Virani et al., 2021). Regular exercise, therefore, is useful in the management of blood pressure.
1.4 Exercise
Inactivity and sedentary lifestyles are risk factors for hypertension (Leitão et al., 2021). As a result, physical activity can enhance the prevention and treatment of cardiovascular diseases by preventing biological and physiological aging of older people (Leitão et al., 2021).
1.5 Conclusion
Cardiovascular diseases are common globally. There is, therefore, the need to develop means of addressing the risk factors to reduce the prevalence. Physical activity through regular exercise is crucial in preventing various cardiovascular conditions, including improving the heart pressure in hypertensive patients. More strategies should therefore be set to help improve the quality of life for individuals at risk or who have developed various cardiovascular conditions
Chapter Two: Methodology
2.1 Overview
This chapter outlines the methods and strategies used to undertake the systematic review. The first section of the chapter addresses the aim, objective, and research question. The inclusion and exclusion criteria that guides the search for literatures are detailed together along with the search strategy. Also, it presents the tools used to evaluate the quality of each study used and the method used for data extraction and synthesis.
2.2 Aim
This systematic review was undertaken to explore the relationship between growing older, reduced exercise and coronary vascular disease. The aim of this dissertation is to critically explore the impact of aerobic exercise for older people with hypertension in lowering the risk of coronary artery disease.
2.3 Objective
1- To evaluate aerobic exercise for older people and its impact in lowering blood pressure.
2- To identify if exercise can lower blood pressure and in turn impact the risk of cardiovascular disease.
2.4 Research question
Does reducing aerobic exercise reduce blood pressure and in turn impact upon the incidence of coronary artery disease among older people?
2.5 Literature Reviews
Systematic review was conducted because it aims to identify, select, and synthesise a focused selection of published research on a particular topic or question in order to compare and contrast findings of previous studies (Peričić, 2019). Hence, review articles provide readers with current knowledge of a research topic (Paul and Criado, 2020). There are several benefits to systematic reviews (SR). To begin with, this process provides a clear and comprehensive overview of available evidence(Chalmers and Glasziou, 2009). Additionally, SRs provide insight into current research gaps in the field and suggest areas for future research(Paul and Criado, 2020). As Gopalakrishnan and Ganeshkumar (2013) advised, evidence-based decisions about individual patients' healthcare and public health policy should be based on the best available research. According to Atkinson and Cipriani (2018) SRs makes informed decisions and developing practice guidelines by synthesising conclusions in areas of ambiguity. Lastly, it is possible to use them to identify questions that are clearly answered by the available evidence, which therefore do not need further investigation(Chalmers and Glasziou, 2009).
2.6 Search Strategy:
The review strategy was originated using the PICO tool(Brown, 2020). PICO includes four elements and it defined as P= Patients\participants, I=intervention, C=comparison, and O=outcome (Wakefield, 2014). The population chosen is the older people with hypertension, intervention is aerobic exercise, and the outcome is reducing the risk of coronary artery disease by managing the blood pressure.
The electronic academic data bases used to search the literature during November 2021 are PubMed and MEDLINE. The reason for choosing MEDLINE as a platform is because it easily accessible through PubMed and consists of over 29 million records(National Library of Medicine, 2022). The references in the included papers were also examined to obtain additional literature. The university library “Al Maktoum Medical Library was accessed as an additional source considering their combined ability to produce relevant evidence. However, the advanced search lacked full text and open access. These databases were suitable for retrieving studies on managing hypertension in older people with aerobic exercise and identifying the effect on cardiovascular health.
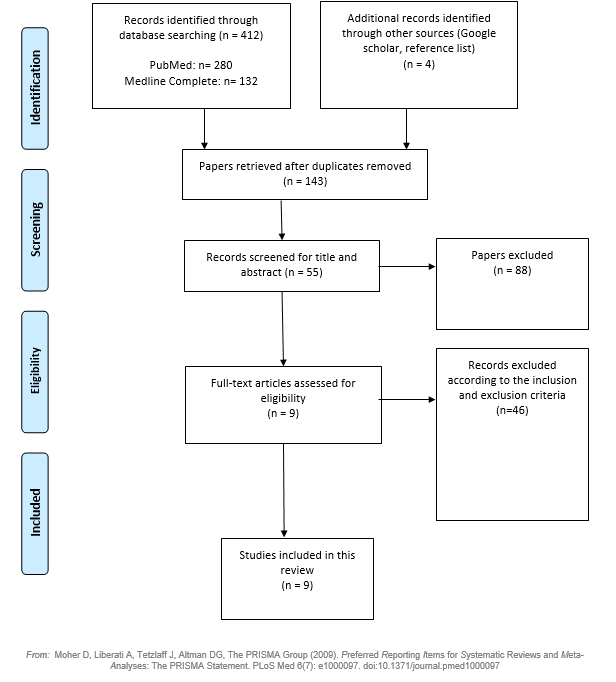
Initially, titles and abstracts of electronic databases and bibliography papers were screened for relevance. Afterwards, the full text was evaluated in detail. Figure 1 is the PRISMA chart, which represent the process of selecting the literature. PRISMA statement stand for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Page et al., 2021). It is an evidence-based minimum set of items for reporting in systematic reviews and meta-analyses (Rethlefsen et al., 2021). It aims to help authors report systematic reviews and meta-analyses more accurately(Rethlefsen et al., 2021).
Initially, 412 titles pf papers were determined from two databases (280 were sourced from PubMed, and 132 from Medline Complete). Meanwhile, a total of four studies were identified from additional sources like google scholar and reference list of included studies. Aveyard et al. (2021) recommended removing duplicate articles and evaluating titles and abstracts when performing a literature review. Of the initial 416 studies, 273 duplicated were removed, leaving 143 papers. Following the review of the titles and abstracts of these 143 papers, 55 papers remained for further evaluation. A full-text version of each of the 55 papers was then sourced and read in full by the author. Only nine papers were relevant to the research aim, resulting in the exclusion of 46 papers. Finally, a total of 9 papers were selected and agreed by the supervisor. The nine full-text papers were then read and analyzed to determine the commonalities and deviations.
Figur1: PRISMA chart
2.7 Inclusion and Exclusion:
Designing high-quality research protocols requires establishing inclusion and exclusion criteria for the study(Patino and Ferreira, 2018). To answer the research question, researchers use inclusion criteria to identify vital characteristics of their target population(Patino and Ferreira, 2018). In order for the readers to understand what the review is trying to achieve and its limitations, researchers must explain their criteria for inclusion and exclusion(Stern et al., 2014). Exclusion criteria, on the other hand, are the aspects of the study participants that satisfy the inclusion criteria but leave the study vulnerable to adverse outcomes (Patino and Ferreira, 2018). In this review, the inclusion require peer-reviewed papers in full text, publication years between January 2015 and December 2022 in English language only. The study types are clinical trial on humans and the participants must be diagnosed with hypertension and their age is 65+. The exercise type chosen is aerobic. For the exclusion criteria, non-English publications were excluded due to a language barrier and lack of translation services. In addition, participants who were not diagnosed with hypertension, publications before 2015, and systematic review, qualitative, and meta-analysis. Participants younger than 65 years old, or younger adults or children. Animal based trials and any types of exercise like resistance were excluded.
2.8 Search terms:
Search terms were developed based on the review topic. The key words in the research including hypertension, high blood pressure, cardiovascular, elderly, exercise, and aerobic. Using the Boolean operators AND and OR, the search terms were combined into strings. Search terms were narrowed with the operator AND, which returned studies containing all the specified terms. For example: elderly and cardio disease. With the operator OR, the searches were expanded to include studies containing any of the search terms – for instance: hypertension OR blood pressure.
Table 1: Search Terms
|
Concept A AND Concept B AND Concept C |
AND Concept D |
||
|
Cardiovascular disease Or cardiovascular |
elderly Or Healthy aging Or Older people Or |
Exercise Or Aerobic exercise Or
|
High blood pressure Or Blood pressure Or Hypertension |
2.9 Quality assessment:
As part of a typical systematic review, individual articles are reviewed for their ability to answer the research question and their quality, which could affect the review's conclusion (Belcher et al., 2016). Table 2 summarise the nine articles assessed. Four papers were assessed by the Critical Appraisal Skills Programme, as Randomised Control Trial(CASP, 2020). The CASP tool is the quality assessment tool used for in this systematic review(Belcher et al., 2016). CASP was selected because it encourages the reviewer to identify the articles' strengths and weaknesses and to determine their external validity and credibility. It has 11 questions, categorises into four sections: section A (“Is the basic study design valid for a randomised controlled trial?”), Section B, (“was the study methodologically sound?”, Section C “What are the results?” and Section D “Will the results help locally?”). Each question has three answers: 'yes', 'no', or 'can't 'tell'. Each 'yes' receives a score of two, each 'no' receives a score of one, and each 'can't tell' receives a score of zero. One study were assessed using the Case Control checklist. It has 11 questions categorise into three sections: Section A(Are the results of the study valid?), Section B(What are the results?), and section C(Will the results help locally?). Three papers were assessed personally as they did not mention the study design. With the supervisor's guidance, they were assessed depending on the study type (qualitative or quantitative) and the data collection process. Secondly, the design was assessed for appropriateness, and the grade was graded upon that.
One study was assessed by ???.
Table 2: Quality evaluation scores
|
NO. |
Study |
Quality appraise tool |
Score |
Quality |
|
1 |
(Venturelli et al., 2015) |
Personal interpretation |
8\10 |
High Quality |
|
2 |
(Prokopets et al., 2021) |
Personal interpretation |
9\10 |
High Quality |
|
3 |
(Gong et al., 2015) |
CASP (RCT) |
7\10 |
Medium quality |
|
4 |
(Saeed et al., 2019) |
Personal interpretation |
7\10 |
Medium quality |
|
5 |
(Reichert et al., 2020) |
quasi-experimental longitudinal study?? (MAAT?JBI?) |
7\10 |
Medium quality |
|
6 |
(Arija et al., 2018) |
CASP (RCT) |
8\10 |
High Quality |
|
7 |
(Ko et al., 2020) |
CASP (RCT) |
7\10 |
Medium quality |
|
8 |
(Gomes et al., 2020) |
CASP (CT) |
7.5\10 |
Medium quality |
|
9 |
(Cramer et al., 2018) |
CASP (RCT |
8\10 |
High Quality |
2.10 Conclusion
This chapter outlines the methodological approach used to conduct this literature review. It addresses the aim, objective, and the research question. In addition, the key terms
Chapter Three: literature Review
3.1 Introduction:
Exercise keeps older people mobile and independent by improving physical functions and reversing the effects of chronic diseases (McPhee et al., 2016). Additionally, there are different types of aerobic exercise that contributes to lowering the blood pressure. Some of the exercise discussed in this chapter include yoga, stretching, aquatic exercise, land exercise including walking. Through a comprehensive review of the literature, this chapter aims to provide an overview of the effects of exercise on blood pressure in older people. Also, this chapter will discuss the emerged themes from the nine papers.
The three emerging themes from the nine papers were:
- The effectiveness of different types of aerobic exercise in lowering blood pressure.
- Effects of exercise-based lowering blood pressure on external factors
- The effectiveness of blood pressure reduction on preventing coronary vascular disease (CVD).
Theme1: The effectiveness of different types of aerobic exercise in lowering blood pressure.
3.1.1 Water versus land exercise training
There are many different types of aerobic exercise or as it called cardio that can be a way of managing the blood pressure. Aquatic exercises are widely used as rehabilitation or preventive therapies specially for older people, as they enable mobilization and muscle strengthening for the lower limbs (Kutzner et al., 2017). In addition, it provides advantages for the elderly because of its lower risk of injury as a result of water buoyancy, and because it guards against joint degradation by reducing weight-bearing loads and reducing the joint load (Kutzner et al., 2017). Moreover, relating this to the study question. Through immersion, aquatic exercise stimulates physiological adjustments that can affect blood pressure and cardiac work, particularly by reducing sympathetic activity and redistributing blood volume from the lower body to the upper body (Reichert et al., 2018). It has been shown that after an acute exercise session, individuals can experience immediate or short-term benefits that last for up to 24 hours. As Gomes et al. (2020) study revealed that the post-exercise hypotension (PEH) for SBP and DBP last for 24 hours post aquatic-based training, which is longer than for land-based training. The post-exercise hypotensive response is considered a vital treatment factor for hypertension (HTN). Additionally, research conducted by Gomes et al. (2020) reveals that exercise in the water during the day lowered systolic blood pressure (SBP) and diastolic blood pressure (DBP) in elderly hypertensive individuals. Similarly, the research conducted by Reichert et al. (2020) showed that aerobic training under water reduced the systolic blood pressure(SBP). The individual blood pressure pretraining was at 130 mmHg, and post eight weeks, it decreased to 129 mmHg, and post 16 weeks, it reached to 124 mmHg. In comparison with pretraining measurements, SBP showed a significant reduction after eight weeks and 16 weeks of training. From pretraining to 16 weeks post training, SBP dropped by 6 mmHg. Likewise, this result is in agreement with Gomes et al. (2020), as the result display that under the water exercise group showed lower SBP and DBP than the land based exercise group.
the study done by Gomes et al. (2020) confirms that the water training resulted in a more remarkable reduction of -10.58 mmHg than that to land aerobic exercise -3.5 mmHg. This shows the effectiveness of the underwater workout compared to the land training.
Gomes et al. (2020) stipulate that the group doing the aquatic exercise had a daytime reduction in BP of 1.0 mmHg in their SBD and 1.5 mmHg in their DBD. The reduction was, however, lower in the group doing the land-based exercises, where there was a reduction of 0.9 mmHg in the SBP and 0.9 mmHg in the DBP. The results showed no significant differences in the nighttime blood pressures. The post-exercise hypotension achieved following aquatic-based exercises was maintained up to 24th after exercise, while that land exercise-induced post-exercise hypotension was maintained to 12th-hour post-exercise.
The BP measurements taken at the 24th hour showed a lower BP in groups that participated in the aquatic-based exercises than those involved in land-based exercises. Gomes et al. (2020) suggest that aquatic training exercises were more effective in lowering the daytime BP of elderly hypertensive patients. It also significantly lowered the resting SDP and DBP compared to individuals who participated in land-based exercises. Lastly, the blood pressure fell rapidly for individuals who participated in aquatic-based exercises, and the post-exercise hypotension lasted longer than for those who participated in the land-based exercises.
Therefore, the study's findings prove that aquatic-based exercises can lower the BP of elderly patients, given their effectiveness compared to land-based exercises. Reichert et al. (2018) further emphasize the need for aquatic training to reduce resting blood pressure for hypertensive patients. The study suggests that aquatic aerobic exercises help reduce the renin-angiotensin and sympathetic activities within the body and subsequently reduce the total peripheral vascular resistance and, eventually, the resting blood pressure.
This was further confirmed in the study, where the intervention showed a progressive reduction in the participants' systolic blood pressure. This ranged from pre-training, after 8 weeks, and after 16 weeks of training as well. The BP values of the participants classified them as stage 1 hypertensive. This, however, changed since, after the 8 weeks of training, the BP values obtained had significantly reduced, and they were qualified for clarification as having normal blood pressure.
There are various forms of exercise in which individuals can participate and help reduce the blood pressure of hypertensive individuals. Some of these exercises, however, are not appropriate for the elderly, given the fragile nature of their bones and joints. This, however, does not lock them out from exercise since they can also benefit from exercise to lower their blood pressure. This is emphasized by Kutzner et al. (2017), who identify aquatic exercise as a form of exercise that is appropriate for the elderly as it prevents joint degradation and other complications which may be associated with weight bearing in the elderly population.
Due to the buoyancy associated with aquatic-based exercises makes it more appropriate for elderly patients compared to land-based exercises, which often cause load on the joints of the elderly individuals, and, subsequently, cause further joint complications. For effective reduction in blood pressure, the exercises should be favorable and appropriate to encourage the participation of the individuals and avoid withdrawals from the exercise program. Due to the complications that may arise due to land-based exercises, the participants will have an increased tendency to fail to comply and then withdraw.
This emphasizes the benefits of an aquatic-based exercise since it enhances mobilization and strengthening of the lower limb muscles and helps ensure minimal joint loading. It can therefore be sustained for a significant duration by the elderly patients, allowing for the outcomes associated with blood pressure reduction to be observed and recorded. The various studies, therefore, associate aquatic-based and land-based exercises with a reduction in blood pressure among the elderly. The studies, however, identify aquatic-based exercises as more feasible and more appropriate in rapidly lowering the blood pressure of hypertensive patients and having a prolonged duration of post-exercise hypotension. Therefore, efforts are required to facilitate aquatic-based exercises for elderly hypertensive individuals, as this will significantly impact the reduction of their blood pressure.
3.1.2 Yoga and relaxing training
For the past years, yoga has been a recommended form of relaxing training aimed at calming the mind and involves spiritual, mental, and physical practices. Yoga and relaxing training help address stress issues, which are one of the risk factors implicated in the development and exacerbation of hypertension. It also helps increase parasympathetic activity and alteration of baroreceptor sensitivities, which are critical in blood pressure reduction and regulation. Therefore, yoga and relaxation training can also be used as a non-pharmacological way of decreasing blood pressure in elderly hypertensive individuals.
According to Cramer et al. (2018), yoga and relaxation training can help lower arterial blood pressure. This can be attributed to the meditation and breathing techniques and, to some extent, the postures. In the study, which involved 90 minutes of yoga training weekly for 12 weeks, the data collectors measured the 24-hour systolic and diastolic blood pressures of all participants who were initially under medications for arterial hypertension. The systolic blood pressure in the group involved in yoga intervention was significantly lower than the control group, with a reduction of up to 3.8 mmHg. The yoga intervention group with yoga postures also recorded a significant reduction in systolic blood pressure, up to 3.2mmHg, slightly below the change observed in the yoga intervention group without posture.
There was, however, no significant reduction in the diastolic blood pressure across the different groups following the yoga intervention. Therefore, Cramer et al. (2018) suggest that only yoga without yoga postures conferred a short-term reduction in resting systolic blood pressure. It, however, should be used as a complementary treatment option for individuals on medications for arterial hypertension, given that it is safe and appropriate for use by the same individuals. The study identifies yoga as one of the lifestyle modifications and exercise techniques that can be used for blood pressure control. Therapeutic yoga, such as meditation and slow breathing, provides relaxation techniques that simultaneously increase parasympathetic activity while simultaneously decreasing sympathetic activity. This has been postulated as the primary mechanism through which yoga exercises reduce arterial blood pressure.
The techniques involved are responsible for reinforcing the parasympathetic system activity, although for the short term. The incorporation of yoga postures, however, does not potentiate the effects of blood pressure reduction, thus the inclusion of breathing and meditation techniques as the principal mechanisms involved in blood pressure reduction when yoga interventions are used rather than yoga postures. Long-term control of arterial blood pressures, however, requires the integration of yoga postures. Such adoption and incorporation of yoga postures can be regarded as isometric training, while the yoga sequences add to the element of aerobic training.
Both aerobic and isometric training can help significantly lowering blood pressure. Therefore, these form the primary mechanisms for long-term control of arterial blood pressure when yoga postures are involved. It is easier to practice and integrate yoga postures into daily activities than meditation and breathing techniques. This makes it easier to achieve the long-term effects of yoga on lowering arterial blood pressures due to the ease of incorporating yoga postures compared to the various techniques such as breathing and meditation. Therefore, participants will likely continue yoga postures, increasing the long-term benefits beyond the study duration. If immediate outcomes are required, the use of yoga breathing and meditation techniques rather than the incorporation of yoga postures should be considered. Either way, there is a considerable benefit in reducing arterial blood pressure.
It is also safe for patients under medication to reduce arterial hypertension. Therefore, it should be considered as one of the lifestyle modification and exercise techniques employed for blood pressure control and prevention of complications. Yoga should therefore be recommended as a complement for reducing arterial blood pressure, even for individuals already on antihypertensive medications, since it is safe and effective.
The main theme focused on the effectiveness of different forms of aerobic exercises in lowering blood pressure. From the studies analyzed, it is clear that exercise is still, by far, an effective way of reducing the risk of developing hypertension and controlling blood pressure for individuals who are already hypertensive. The various studies also highlighted some of the most appropriate exercises elderly patients can use to control their blood pressure properly.
Some of the identified forms of appropriate, safe, and effective exercises in lowering blood pressure from the various studies include; aquatic-based exercises and yoga with or without postures depending on the duration of outcomes required. The studies, therefore, confirm why it is important to encourage the elderly who are hypertensive to adopt an exercise schedule since this is beneficial in lowering their blood pressure and preventing the complications associated with poorly controlled blood pressure, such as stroke, heart attacks, and even deaths.
Theme2: Effects of exercise-based lowering blood pressure on external factors
Many elderly individuals develop hypertension globally. Most hypertensive individuals are on regular follow-up and antihypertensive medications as the primary mechanism of blood control. Exercise has, however, not gained much incorporation into practice as a way of controlling blood pressure, especially within the elderly age group, where the range of functionality is reduced due to the advancing age (Leitão et al., 2021). Despite exercise being regarded as an intervention useful in the control of blood pressure, the majority of the elderly population does not engage in exercise. Despite being the most vulnerable age group to be affected by multiple chronic conditions such as hypertension, exercise could lower the associated risk.
Most older individuals, therefore, tend to come up with excuses for not engaging in exercises, such as the fact that exercise may increase their risk of falling, from which they will end up hurt or develop further complications. Some elderly individuals also believe that they are too old; hence exercise would not significantly affect their well-being (Leitão et al., 2021). Besides, some believe that engaging in some exercise is not good for individuals with chronic conditions. These beliefs, which can be regarded as misconceptions, prevent these elderly individuals from exercising.
As such, most of them experience worse health outcomes, which could have been prevented if they exercised regardless of their age (Moraes-Silva et al., 2017). Various studies have, however, brushed off these misconceptions, as they have identified the benefits of exercise among the elderly in improving their health outcomes and well-being. Moraes-Silva et al. (2017) confirm that exercise is a lifestyle modification factor that can help lower the risk of developing cardiovascular diseases such as hypertension and optimize the treatment and prevent the development of complications that can significantly lower the quality of life of the affected individuals.
Therefore, there is a need to debunk the existing myths and misconceptions elderly individuals may have regarding exercise. This can be achieved through proper education of the elderly population. It will help them change the negative attitude that the elderly have towards exercise and help them develop a positive mindset which will help them to exercise appropriately, thus reducing the risk of developing various chronic conditions (Leitão et al., 2021).
Education Wise:
As aforementioned, the majority of the elderly population have various misconceptions which prevent them from engaging in exercises, which, when appropriately done, can help improve their health outcomes. Addressing these misconceptions, therefore, requires adequate patient enlightenment through patient health education. Individuals should be aware that exercise helps prevent various chronic health conditions that may lower their quality of life (Leitão et al., 2021). Discussing this with the individuals will help address the myths that exercise is not good for them due to their chronic health conditions.
Educating the patients that exercise does not lead to falls will help them improve their balance and coordination, reducing their fall risk. This will also help in encouraging more of them to participate in exercise since they will be able to overcome the previously existing myths and misconceptions. During patient education, it is also important that they are informed on how the exercise will be coordinated to ensure it is safe and manageable for them (Moraes-Silva et al., 2017). Having someone watching the elderly as they exercise will help in preventing injuries that may result from exercising. Besides, choosing the most appropriate exercises that do not put too much pressure on the individual's system, especially the heart, joints, and respiratory system, will also help ensure that the exercise prescribed is appropriate and effective in improving the individual's well-being (Leitão et al., 2021).
Educating the patients also helps in identifying the concerns they may have and identifying the barriers that prevent them from exercising. Addressing the individual's concerns and needs help in developing plans that will address the various concerns and encourage them to participate in the exercise, from light exercises as they advance, depending on their levels of functionalities. Such exercises will help improve the well-being of hypertensive individuals, as appropriate exercises will help improve the function of their cardiovascular system, thereby helping lower resting blood pressure (Moraes-Silva et al., 2017). Appropriate exercises also help complement the treatment options, thereby improving blood pressure control, preventing complications, and subsequently improving the health outcome and quality of life of the affected individuals (Moraes-Silva et al., 2017).
Exercise Time:
It is universally recommended that those with HTN exercise for 30 minutes of vigorous exercise or 60 minutes of moderate-intensity four or five days a week to reduce blood pressure (Moraes-Silva et al., 2017). The total duration of exercise for these individuals should be 150 minutes or more per week, a time duration that is consistent with the recommendations for the general population. Aerobic exercises for approximately 15 minutes consisting of light to moderate intensity exercise help achieve post-exercise hypotension for the remainder of the day. The exercise duration should be interspersed throughout the day, with the duration being modified depending on the patient's level of cardiovascular function. This will help ensure that the individuals' cardiovascular system is not strained too much to the extent that its functionality is compromised, which can lead to further complications (Leitão et al., 2021).
The main factor in achieving a proper exercise schedule for the elderly is time to do the exercises and adherence. This, therefore, requires that the various bouts of exercise are interspersed throughout the day to help ensure that the individuals adhere well to the schedule (Venturelli et al., 2015). This can also be achieved by educating the caregiver on the timing of the exercises, the types of exercises, and the duration of exercise in which the individual should engage at different times. Emphasis should also be placed on the need for a caregiver or instructor to be around at the time of exercise to help prevent any complications such as patient falls or inappropriate exercises that may further put the life of the individual at risk given their preexisting cardiovascular condition.
Theme3: The effectiveness of blood pressure reduction on preventing coronary vascular disease (CVD).
Conclusion:
Across continents, this study found that exercise significantly lowers blood pressure in older adults. As a result, elderly with hypertension may benefit from regular physical activity.
Arija, V., Villalobos, F., Pedret, R., Vinuesa, A., Jovani, D., Pascual, G. & Basora, J. 2018. Physical activity, cardiovascular health, quality of life and blood pressure control in hypertensive subjects: randomized clinical trial. Health and quality of life outcomes, 16, 1-11.
Atkinson, L. Z. & Cipriani, A. 2018. How to carry out a literature search for a systematic review: a practical guide. BJPsych Advances, 24, 74-82.
Aveyard, H., Payne, S. & Preston, N. 2021. A Postgraduate's Guide to Doing a Literature Review in Health and Social Care, 2e.
Battaglini, D., Robba, C., Lopes da Silva, A., dos Santos Samary, C., Leme Silva, P., Dal Pizzol, F., Pelosi, P. & Rocco, P. R. M. 2020. Brain–heart interaction after acute ischemic stroke. Critical Care, 24, 1-12.
Belcher, B. M., Rasmussen, K. E., Kemshaw, M. R. & Zornes, D. A. 2016. Defining and assessing research quality in a transdisciplinary context. Research Evaluation, 25, 1-17.
Brown, D. 2020. A review of the PubMed PICO tool: using evidence-based practice in health education. Health promotion practice, 21, 496-498.
CASP. 2020. Randomised Controlled Trial Checklist [Online]. Available: https://casp-uk.net/casp-tools-checklists/ [Accessed 17\07 2022].
Chalmers, I. & Glasziou, P. 2009. Avoidable waste in the production and reporting of research evidence. The Lancet, 374, 86-89.
Cramer, H., Sellin, C., Schumann, D. & Dobos, G. 2018. Yoga in arterial hypertension: A three-armed, randomized controlled trial. Deutsches Ärzteblatt International, 115, 833.
Fuchs, F. D. & Whelton, P. K. 2020. High blood pressure and cardiovascular disease. Hypertension, 75, 285-292.
Gomes, S. G., Da Silva, F. F., Souza, P. M., Coelho, D. B., Oliveira, E. C., Nascimento-Neto, R. M., Lima, W., Becker, L. K. & Júnior, F. A. 2020. The effects of aquatic and land exercise on resting blood pressure and post-exercise hypotension response in elderly hypertensives. Cardiovascular Journal of Africa, 31, 116-122.
Gong, J., Chen, X. & Li, S. 2015. Efficacy of a community-based physical activity program KM2H2 for stroke and heart attack prevention among senior hypertensive patients: a cluster randomized controlled phase-II trial. PLoS One, 10, e0139442.
Gopalakrishnan, S. & Ganeshkumar, P. 2013. Systematic reviews and meta-analysis: understanding the best evidence in primary healthcare. Journal of family medicine and primary care, 2, 9.
Hajat, C. & Stein, E. 2018. The global burden of multiple chronic conditions: a narrative review. Preventive medicine reports, 12, 284-293.
Kaptoge, S., Pennells, L., De Bacquer, D., Cooney, M. T., Kavousi, M., Stevens, G., Riley, L. M., Savin, S., Khan, T. & Altay, S. 2019. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. The Lancet Global Health, 7, e1332-e1345.
Ko, J., Deprez, D., Shaw, K., Alcorn, J., Hadjistavropoulos, T., Tomczak, C., Foulds, H. & Chilibeck, P. D. 2020. Stretching is Superior to Brisk Walking for Reducing Blood Pressure in People With High–Normal Blood Pressure or Stage I Hypertension. Journal of Physical Activity and Health, 18, 21-28.
Kutzner, I., Richter, A., Gordt, K., Dymke, J., Damm, P., Duda, G. N., Günzl, R. & Bergmann, G. 2017. Does aquatic exercise reduce hip and knee joint loading? In vivo load measurements with instrumented implants. PloS one, 12, e0171972.
Leitão, L., Marocolo, M., Souza, H. L. d., Arriel, R. A., Vieira, J. G., Mazini, M., Louro, H. & Pereira, A. 2021. Can Exercise Help Regulate Blood Pressure and Improve Functional Capacity of Older Women with Hypertension against the Deleterious Effects of Physical Inactivity? International Journal of Environmental Research and Public Health, 18, 9117.
Lung, N. H. & Institute, B. 2011. Systolic Blood Pressure Intervention Trial (SPRINT).
McPhee, J. S., French, D. P., Jackson, D., Nazroo, J., Pendleton, N. & Degens, H. 2016. Physical activity in older age: perspectives for healthy ageing and frailty. Biogerontology, 17, 567-580.
Modesti, P. A., Reboldi, G., Cappuccio, F. P., Agyemang, C., Remuzzi, G., Rapi, S., Perruolo, E., Parati, G. & Settings, E. W. G. o. C. R. i. L. R. 2016. Panethnic differences in blood pressure in Europe: a systematic review and meta-analysis. PloS one, 11, e0147601.
Moraes-Silva, I. C., Mostarda, C. T., Silva-Filho, A. C. & Irigoyen, M. C. 2017. Hypertension and exercise training: evidence from clinical studies. Exercise for Cardiovascular Disease Prevention and Treatment. Springer.
NIH. 2022. MEDLINE: Overview [Online]. Available: https://www.nlm.nih.gov/medline/medline_overview.html [Accessed 25/07 2022].
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A. & Brennan, S. E. 2021. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. bmj, 372.
Patino, C. M. & Ferreira, J. C. 2018. Inclusion and exclusion criteria in research studies: definitions and why they matter. Jornal Brasileiro de Pneumologia, 44, 84-84.
Paul, J. & Criado, A. R. 2020. The art of writing literature review: What do we know and what do we need to know? International Business Review, 29, 101717.
Peričić, T. 2019. Why systematic reviews matter [Online]. Available: https://www.elsevier.com/connect/authors-update/why-systematic-reviews-matter [Accessed 13/07 2022].
Pickering, T. G., White, W. B. & Group, A. S. o. H. W. 2008. When and how to use self (home) and ambulatory blood pressure monitoring. Journal of the American Society of hypertension, 2, 119-124.
Prokopets, T., Osipov, A., Lyakh, V., Ratmanskaya, T., Orlova, I., Vinnik, Y., Galimova, A. & Kudryavtsev, M. 2021. Effect of healthful physical training on functional status in physically inactive middle-aged women with hypertension. Journal of Physical Education and Sport, 21, 2199.
Reichert, T., Costa, R. R., Barroso, B. M., da Rocha, V. d. M. B., Delevatti, R. S. & Kruel, L. F. M. 2018. Aquatic training in upright position as an alternative to improve blood pressure in adults and elderly: A systematic review and meta-analysis. Sports Medicine, 48, 1727-1737.
Reichert, T., Costa, R. R., Barroso, B. M., da Rocha, V. d. M. B., Oliveira, H. B., Bracht, C. G., de Azevedo, A. G. & Kruel, L. F. M. 2020. Long-Term Effects of Three Water-Based Training Programs on Resting Blood Pressure in Older Women. Journal of Aging and Physical Activity, 28, 962-970.
Rethlefsen, M. L., Kirtley, S., Waffenschmidt, S., Ayala, A. P., Moher, D., Page, M. J. & Koffel, J. B. 2021. PRISMA-S: an extension to the PRISMA statement for reporting literature searches in systematic reviews. Systematic reviews, 10, 1-19.
Saeed, S., Mancia, G., Rajani, R., Parkin, D. & Chambers, J. B. 2019. Hypertension in aortic stenosis: relationship with revealed symptoms and functional measures on treadmill exercise. Journal of Hypertension, 37, 2209-2215.
Sardarinia, M., Akbarpour, S., Lotfaliany, M., Bagherzadeh-Khiabani, F., Bozorgmanesh, M., Sheikholeslami, F., Azizi, F. & Hadaegh, F. 2016. Risk factors for incidence of cardiovascular diseases and all-cause mortality in a middle eastern population over a decade follow-up: Tehran lipid and glucose study. PloS one, 11, e0167623.
Saxena, T., Ali, A. O. & Saxena, M. 2018. Pathophysiology of essential hypertension: an update. Expert review of cardiovascular therapy, 16, 879-887.
Stern, C., Jordan, Z. & McArthur, A. 2014. Developing the review question and inclusion criteria. AJN The American Journal of Nursing, 114, 53-56.
Subirana, M., Solá, I., Garcia, J. M., Gich, I. & Urrútia, G. 2005. A nursing qualitative systematic review required MEDLINE and CINAHL for study identification. Journal of clinical epidemiology, 58, 20-25.
Timmis, A., Townsend, N., Gale, C. P., Torbica, A., Lettino, M., Petersen, S. E., Mossialos, E. A., Maggioni, A. P., Kazakiewicz, D. & May, H. T. 2020. European Society of Cardiology: cardiovascular disease statistics 2019. European heart journal, 41, 12-85.
Venturelli, M., Cè, E., Limonta, E., Schena, F., Caimi, B., Carugo, S., Veicsteinas, A. & Esposito, F. 2015. Effects of endurance, circuit, and relaxing training on cardiovascular risk factors in hypertensive elderly patients. Age, 37, 1-13.
Virani, S. S., Alonso, A., Aparicio, H. J., Benjamin, E. J., Bittencourt, M. S., Callaway, C. W., Carson, A. P., Chamberlain, A. M., Cheng, S. & Delling, F. N. 2021. Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation, 143, e254-e743.
Wakefield, A. 2014. Searching and critiquing the research literature. Nursing Standard (2014+), 28, 49.
Weber, M. A., Schiffrin, E. L., White, W. B., Mann, S., Lindholm, L. H., Kenerson, J. G., Flack, J. M., Carter, B. L., Materson, B. J. & Ram, C. V. S. 2014. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. The journal of clinical hypertension, 16, 14.
Williams, B., Mancia, G., Spiering, W., Agabiti Rosei, E., Azizi, M., Burnier, M., Clement, D. L., Coca, A., De Simone, G. & Dominiczak, A. 2018. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). European heart journal, 39, 3021-3104.
